Dr Rajiv Desai
An Educational Blog
ORGAN DONATION & TRANSPLANTATION (ODT)
Organ Donation & Transplantation (ODT):
____

Jemima Layzell died of a brain aneurysm in 2012 and her organ donations have helped eight people including five children.
____
Prologue:
In 1894, the surgeon Otto Lanz (1865–1935) warned his colleagues not to scoff at a treatment “which aims at replacing the organ that has lost its function in the organism”. Today, no one would doubt the seriousness of a surgeon who treats a disease by replacing an organ. However, it was only around 1900 that the idea of organ replacement became self-evident. The introduction of antibiotics, massive vaccinations of the general population to prevent infectious diseases, and organ transplantation may be considered the miracles of twentieth century medicine. Organ transplantation is the best therapy for terminal and irreversible organ failure. Transplantation has given many a new lease on life and, to many more, an extension that would have otherwise been impossible. Organ transplantation has progressed tremendously with improvements in surgical methods, organ preservation, and pharmaco-immunologic therapies and has become a critical pathway in the management of severe organ failure worldwide. The major sources of organs are deceased donors after brain death; however, a substantial number of organs come from live donations, and a significant number can also be obtained from deceased donors after cardio-circulatory death. Yet, despite progress in medical, pharmacologic, and surgical techniques, shortage of organs is a worldwide problem that needs to be addressed internationally at the highest possible levels. This particular field involves medical ethics, religion, and society behavior & beliefs. The issue of consent for organ donation after death remains controversial. Some of the critical ethical issues that require aggressive interference are organ trafficking, payments for organs, and the delicate balance in live donations between the benefit to the recipient and the possible harm to the donor. Organ transplantation also faces challenges of biological nature, such as organ rejection from the recipient. Almost anyone can register to be organ donor, regardless of age or medical history. One organ donor can save up to eight lives. The same donor can also improve lives of up to 50 people by donating tissues and eyes. Organ recipients are selected based primarily on medical need, location and compatibility. In 2014, 119,873 solid organ transplants were performed worldwide but the annual number of organ transplants represents less than 10% of the global needs. Organ shortage leads to deaths and poor quality of life for those on the waiting list. More than 115,000 people in the United States are waiting for organ transplant and another name is added to the waiting list every 10 minutes. Almost 96,000 individuals in U.S. die each year waiting for a new kidney. In India every year nearly 500,000 people die because of non-availability of organs. August 13th is observed as Organ Donation Day every year; but there is no better time than today to sign up as an organ donor.
______
Abbreviations and synonyms:
DBD = donation after brain death
DCD = donation after cardiac death/ circulatory death/ cardio-circulatory death
DDR = dead donor rule
OPO = organ procurement organization
ECD = Expanded/extended criteria donor
OPTN = Organ Procurement and Transplantation Network
UNOS = United Network for Organ Sharing
HSCT = Hematopoietic stem cell transplantation
BMT = blood marrow transplantation
AST = American Society of Transplantation
PMP = per million population (per year)
DPMP = Donors per Million Population (per year)
MHC = Major histocompatibility complex
HLA = Human leukocyte antigens
GVHD = Graft- versus- host disease
APC = Antigen-presenting cells
CDC = complement-dependent cytotoxicity (crossmatch)
AMR = Antibody mediated rejection
PRA = Panel Reactive Antibody
Treg = T regulatory cells
VCA = Vascularized composite allograft
ATG = Antithymocyte globulin
IVIG = Intravenous immunoglobulin
siRNA = small interfering RNA
DSA = Donor specific anti-HLA antibodies
______
Terminology in organ donation & transplantation (ODT):
Donation: Donation refers to donating human cells, tissues, or organs intended for human applications. The donor is a human being, living or deceased, who is a source of cells, tissues, or organs for the purpose of transplantation.
Transplantation: Transplantation refers to transfer (engraftment) of human cells, tissues, or organs from a donor to a recipient with the aim of restoring function(s) of the body.
Living Donors: Living donor is a living human being from whom cells, tissues, or organs have been removed for the purpose of transplantation. Living donors are often close relatives of the recipient, but may sometimes be a spouse, friend or even someone who is unknown to the recipient (non-directed donor).
Deceased Donors: Individuals whose organs and/or tissues are donated at the time of their death. Deceased donors are sometimes called cadaveric donors or non-living donors.
Actual Donors: Actual organ donors are those with at least 1 organ successfully transplanted into a recipient. Potential Donors: Potential donors are patients who died in hospitals and who were clinically eligible to be organ donors. To be clinically eligible, patients typically died after experiencing severe brain damage (leading to brain or cardio-circulatory death), were mechanically ventilated at or near the time of death and had no medical contraindications to donation.
Donation after Brain Death (DBD): Most deceased organ donation occurs after brain death. At least 2 physicians must determine brain death based on a standard list of neurological criteria.
Donation after Cardio-circulatory Death: This involves donation from a patient with a severe brain injury who does not meet the criteria for brain death but who has no chance of recovery and is removed from life-sustaining therapy with the consent of his or her family. Accordingly death is declared 5 minutes after the heart stops beating. Donation after cardio-circulatory death (DCD) is also known as non–heart beating donation.
Donors per Million: This is the number of actual or potential donors per million people per year. It allows for more comparable measurement by province and/or country by adjusting for differences in population sizes.
Exclusion Criteria: These are medical contraindications that would prevent a person with a brain death or cardiocirculatory death from being considered for organ donation.
Expanded criteria donor (ECD): Deceased donor who falls outside the standard criteria used to determine donor suitability.
Donor Registries: A confidential electronic database in which individuals can enter and store their wish to be an organ and tissue donor at the time of their death. Many states have donor registries. Registering with one of these agencies confirms your donation wishes.
Graft Survival: The length of time an organ functions successfully after being transplanted. Grafting refers to a surgical procedure to move tissue from one site to another on the body, or from another creature, without bringing its own blood supply with it. Instead, a new blood supply grows in after it is placed. A similar technique where tissue is transferred with the blood supply intact is called a flap. However in this article, ‘Graft’ means transplanted organ or ‘transplant’.
Organ Procurement Organizations (OPOs): Organizations that recover organs from deceased donors and deliver them to transplant centers where a recipient “match” is located.
Organ Procurement and Transplantation Network (OPTN): A national transplant network, established by an act of U.S. Congress, which maintains the national computer registry for matching donated organs to patients on the waiting list. The OPTN is administered by the United Network for Organ Sharing (UNOS).
Solid Organ Transplants: These types of transplants include the following: kidney, liver, intestines, heart, lung and pancreas.
Immunosuppression: Suppression of the immune system and its ability to fight infection. Immunosuppression may result from certain diseases, such as AIDS or lymphoma, or from certain drugs, such as some of those used to treat cancer. Immunosuppression may also be deliberately induced with drugs, as in organ transplantation, to prevent the rejection of a transplant.
_____
_____
Introduction to organ donation & transplantation (ODT):
Organ donation is when a person allows an organ of theirs to be removed, legally, either by consent while the donor is alive or after death with the assent of the next of kin. Donation may be for research, or, more commonly healthy transplantable organs and tissues may be donated to be transplanted into another person. Common transplantations include: kidneys, heart, liver, pancreas, intestines, lungs, bones, bone marrow, skin, and corneas. Some organs and tissues can be donated by living donors, such as a kidney or part of the liver, part of the pancreas, part of the lungs or part of the intestines, but most donations occur after the donor has died. As of February 2, 2018, there were 115,085 people waiting for life-saving organ transplants in the US. Of these, 74,897 people were active candidates waiting for a donor. The most important fact to know about organ donation is that many people who need a new kidney or liver or heart never get one.
_
- Organ transplants – replacing diseased organs, such as hearts, lungs, livers, pancreases and kidneys.
- Cell transplants – replacing damaged or destroyed cells in diseases such as diabetes, Alzheimer’s and Parkinson’s disease
- Tissue transplants – skin grafts, cornea transplants or bone transplants.
- Bridging transplants – providing organ function externally to patients with organ failure.
_
Transplants and grafts:
Transplant, also called graft or organ transplant, in medicine, is a section of tissue or a complete organ that is removed from its original natural site and transferred to a new position in the same person or in a separate individual. The term, like the synonym graft, was borrowed from horticulture. Both words imply that success will result in a healthy and flourishing graft or transplant, which will gain its nourishment from its new environment.
_
Transplants of animal tissue have figured prominently in mythology since the legend of the creation of Eve from one of Adam’s ribs. Historical accounts of surgical tissue grafting as part of the cure of patients date back to the early Indian surgeons who, about the beginning of the 6th century BCE, developed techniques for reconstructing noses from skin flaps taken from the patient’s arm. This method was introduced into Western medicine by Italian surgeon Gaspare Tagliacozzi in the 16th century. The flap was left attached to the arm for two to three weeks until new blood vessels had grown into it from the nose remnant. The flap was then severed and the arm freed from the reconstructed nose. It was found that extremely thin pieces of skin could be cut free and would obtain enough nourishment from the serum in the graft bed to stay alive while new blood vessels were being formed. This free grafting of skin, together with the flap techniques already mentioned, constituted the main therapeutic devices of the plastic surgeon in the correction of various types of defects. Skilled manipulations of such grafts produced surprising improvements in the appearance of those born with malformed faces and in the disfigurements resulting from severe burns. Cornea, which structurally is a modified form of transparent skin, can also be free grafted, and corneal grafts have restored sight to countless blind eyes. Blood transfusion can be regarded as a form of tissue graft. The blood-forming tissues—bone marrow cells—can also be transplanted. If these cells are injected into the bloodstream, they home to the marrow cavities and can become established as a vital lifesaving graft in patients suffering from defective marrow.
_
The chief distinguishing feature of organ and limb grafts is that the tissues of the organ or limb can survive only if blood vessels are rapidly joined (anastomosed) to blood vessels of the recipient. This provides the graft with a blood supply before it dies from lack of oxygen and nourishment and from the accumulation of poisonous waste products. As can be seen from the examples cited, living-tissue grafts may be performed for a variety of reasons. Skin grafts can save life in severe burns, can improve function by correcting deformity, or can improve appearances in a cosmetic sense, with valuable psychological benefits. Organ grafts can supply a missing function and save life in cases of fatal disease of vital organs, such as the kidney.
_
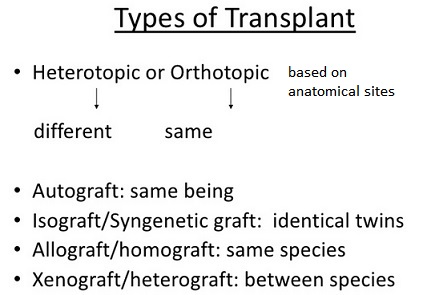
A tissue removed from one part of the body and transplanted to another site in the same individual is called an autograft. Autografts cannot be rejected. Similarly, grafts between identical twins or highly inbred animals—isografts—are accepted by the recipients indefinitely. Grafts from a donor to a recipient of the same species—allografts or homografts—are usually rejected unless special efforts are made to prevent this. Grafts between individuals of different species—xenografts or heterografts—are usually destroyed very quickly by the recipient.
_
Tissue or organ grafts may be transplanted to their normal situation in the recipient and are then known as orthotopic—for example, skin to the surface of the body. Alternatively, they may be transplanted to an abnormal situation and are then called heterotopic—for example, kidneys are usually grafted into the lower part of the abdomen instead of into the loin (the back between the ribs and the pelvis), as this is more convenient. If an extra organ is grafted, it is called auxiliary or accessory—for example, a heterotopic liver graft may be inserted without removal of the recipient’s own liver.
_
Grafts are usually performed for long-term effects. Occasionally, the limited acceptance of a skin allograft may be lifesaving by preventing loss of fluid and protein from extensive burned surface in severely ill patients. The graft also provides a bacteria-proof covering so that infection cannot occur. When the allograft is removed or rejected, the patient may be sufficiently recovered to receive permanent autografts. Certain tissues, including bone, cartilage, tendons, fascia, arteries, and heart valves, can be implanted even if their cells are dead at the time of implantation or will be rejected shortly thereafter. These are structural implants rather than true grafts or transplants. They are more akin to the stick to which a rose is attached for support—although their support is essential, their function does not depend on biological processes. In fact, xenografts or inert manufactured devices may often be equally suitable substitutes.
______
Organ transplantation:
The transplantation of an organ from one body to another is known as the organ transplant. The person who gives the organ is called the donor while the one who receives is called the recipient. Organ transplant is done to replace the recipient’s damaged organ with the working organ of the donor so that the recipient could function normally. There are no cut-off ages for donating organs. Organs have been successfully transplanted from newborns and people older than 80. The conditions that will absolutely exclude donation are HIV, active cancer and systemic infection.
_
By definition an organ transplant is the moving of a whole or partial organ from one body to another (or from a donor site on the patient’s own body), for the purpose of replacing the recipient’s damaged or failing organ with a working one from the donor site. Organ transplants can be categorized as “life-saving”, while tissue transplants are “life-enhancing”. Organs that can be transplanted are the heart, kidneys, liver, lungs, pancreas, and intestine. Tissues include bones, tendons, cornea, heart valves, veins, and skin. Worldwide, the kidneys are the most commonly transplanted organs, followed by the liver and then the heart. Cornea and musculoskeletal grafts are the most commonly transplanted tissues; these outnumber organ transplants by more than tenfold. Hematopoietic stem cell transplantation (HSCT), often called blood marrow transplantation (BMT), is another common tissue transplantation procedure.
A transplant is an organ, tissue or a group of cells removed from one person (the donor) and surgically transplanted into another person (the recipient or host) or moved from one site to another site in the same person. Transplants – such as a liver transplant – can save lives. They can also restore function to improve quality of life. For example, transplanting the clear tissue that covers the eye (cornea) is not necessary for life, but can restore sight.
_
The donated organ may be from a deceased donor (previously referred to as cadaveric), a living donor, or an animal. In some cases an artificial organ is used. Cadaveric organ donation involves removing organs from a recently deceased donor (brain dead, or dead via circulatory death). Living organ donation involves the donation of one of a paired organ (such as kidneys) or a portion of an organ (such as a lobe of the liver or lung). The donor’s organ system is still able to function after the donation. Living donors are often related to the patient, but that is not always the case.
_
Not all people who die can be organ donors. In the case of people who die of brain death or cardiac death in hospital ICU, they can donate all tissues and many organs (kidneys, liver, lungs etc). However, most people die due to cardiac arrest outside hospital setup regardless of the condition or situation that causes the heart function to stop. For these cases, they can only donate tissues such as corneas. Whatever the case, it is always necessary to carry out a medical examination to assess the condition of the body and each organ.
_
Living tissue deteriorates rapidly when it loses its blood supply, and organs need to be cooled and transported for implantation into the recipient within a limited number of hours. Short transfer time, entailing removal of organs from ‘beating heart’ donors, was made possible by the acceptance of ‘brain stem death’ as death. While most organs must be used between 6 and 72 hours after removal from a donor’s body, tissues such as corneas, skin, heart valves, bone, tendons, ligaments, and cartilage can be preserved and stored for use later. Tissue may be recovered from donors who die of circulatory death, as well as of brain death – up to 24 hours past the cessation of heartbeat unlike organs which must be recovered immediately after cardiac death. Unlike organs, most tissues (with the exception of corneas) can be preserved and stored for up to five years, meaning they can be “banked”.
_
Organ transplantation has a key role in medicine worldwide and has become an essential treatment modality in saving and prolonging lives in a wide variety of clinical conditions. Kidney, heart, liver, lung, and pancreas are among the vital organs that are routinely used for transplantation, but many other organs that draw less public attention such as small bowel, skin, ligaments, bones, and cornea are used in various clinical conditions to provide temporary or permanent relief for various clinical conditions. In general, organ transplantation saves lives, prolongs survival, and increases the quality of life. Kidney transplantation has been proven to have a survival advantage over hemodialysis, accompanied by a marked increase in the quality of life. In general, organ implantation is co-ordinated via regional or national allocation programs, which set up the priorities for organ allocation and provide the essential logistics and laboratory support for the transplantation process. These organs can be preserved for a relatively short period of time, and therefore mechanisms for immediate organ allocation, once a donor is identified, are critical.
_
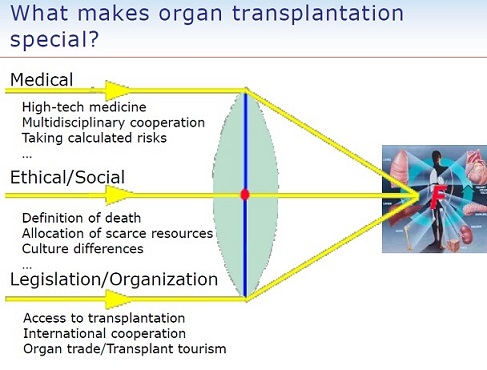
Organ transplantation is one of the most complex procedures in medicine for several reasons. First and foremost, it involves dealing with the medical aspects of the recipient patient in parallel to dealing with a matched donor in case of a living donor or his family for a deceased donor. Whether involving a deceased or a living donor, the ethical rules that wrap the process of organ transplantation are complex and often convoluted by ethical and religious nuances. Ethical issues with the timely and unequivocal definition of death are among the most debatable and complex dilemmas in medicine, and the public opinion is often skewed by religious and cultural influences and ethical standards that vary between different cultures and religions. Transplantation raises a number of bioethical issues, including the definition of death, when and how consent should be given for an organ to be transplanted, and payment for organs for transplantation. Other ethical issues include transplantation tourism and more broadly the socio-economic context in which organ procurement or transplantation may occur. A particular problem is organ trafficking. On top of that, the field of transplantations is faced with a worldwide shortage of organs, and this mandates the need to guard the ethical standard of medical priorities for those patients that depend on the transplantation to save their lives.
_
Transplantation medicine is one of the most challenging and complex areas of modern medicine. Rejection of a transplant occurs in instances where the recipient immune system identifies the transplant as foreign, triggering a response that will ultimately destroy the transplanted organ or tissue. Some of the key areas for medical management are the problems of transplant rejection, during which the body has an immune response to the transplanted organ, possibly leading to transplant failure and the need to immediately remove the organ from the recipient. When possible, transplant rejection can be reduced through serotyping to determine the most appropriate donor-recipient match and through the use of immunosuppressant drugs. The intensity of the immune response against the organ or tissue, also commonly referred to as the graft, will depend on the type of graft being transplanted and the genetic disparity between the donor and recipient. To reduce the possibility of rejection, the donor and recipient are carefully matched for immune compatibility prior to transplantation. However, the small pool of eligible donors can make it difficult to find a donor-recipient match and there will always be a degree of rejection against the graft. A critical undersupply of donated organs means that waiting lists for transplants are extremely long. Patients needing a kidney transplantation, for example, wait on average 944 days (more than two and a half years) for a life-saving transplant. In the UK, there is still around a seven to one discrepancy between those requiring a kidney transplant and the number of donors. There were 6,943 patients registered for organ transplant in the UK as of March 2015. Unfortunately, 479 of these patients died during 2015/16 whilst waiting for a transplant due the small pool of transplantable organs. These figures underline the value of every organ and highlight the importance of a successful transplantation and maintaining long-term transplant survival. Manipulation of the immune system can support long term survival of the graft ensuring that every transplant is as successful as possible.
_
Organ donation and transplantation (ODT) is a modern day success story: everything about it can be seen in a positive light. For the donor and their relatives, something good has emerged from a disaster. For the recipient, there is the opportunity for a new independent life, free from many of the constraints of supportive therapy. For the medical profession, there is an opportunity to bring about a cure for an otherwise intractable acute or chronic disease, and for society as a whole, it provides an exceedingly cost-effective solution. The ‘Holy Grail’ of treatment for organ failure remains the ability to regenerate individual organs for an individual patient using stem cell technology. However, ODT is currently the most realistic option for chronic organ failure, which (particularly in the case of renal failure) can occur in an otherwise fit and healthy individual. Indeed, solid organ and tissue transplantation, either singly or combined, is being used for increasingly complex diseases and situations way beyond those currently considered usual, such as the kidney, liver, pancreas, heart, and lung. Furthermore, composite tissue transplants (e.g. involving the trachea, the face, or a whole limb) are being developed; undoubtedly, these will become more routine in the future.
_
Experts say a number of myths and misconceptions keep others from making this life-saving gift. One common fear is that hospitals might not work as hard to save your life if they want your organs for transplant. Experts say that is totally false. If you’re in an accident the first thing is they’re going to save your life, not look for your organ donor designation on your license. Another misconception many people have is that organ donation violates religious principles. In fact, organ donation is consistent with most major religions. And one more myth the experts would like to lay to rest: the idea that you may be too old to donate. The U.S. Department of Health and Human Services says there is no predetermined cut-off age for donating organs. Whether a person is a suitable donor depends on their physical condition, not age.
_______
The organ transplantation community faces three main issues:
- Lack of organs
Of the +120,000 people waiting for an organ in the U.S., an average of 22 people will die a day waiting. The number of organs sufficient for transplantation from deceased and living donors has plateaued.
- Organ transplantation failure
Approximately 50 percent of all transplanted organs will experience failure within five to ten years, typically due to organ rejection or complications from immunosuppression drugs. This leads to the recipient needing a second transplant, which is a very challenging and risky procedure.
- Lack of research funding
Organ transplantation research is severely underfunded. In fact, in comparison to efforts to fight other serious medical conditions, transplantation research has almost no public support.
Organ transplantation is a life-saving treatment – but not a cure. Beyond the transplant recovery lies a lifetime of medications and therapies to maintain the recipient’s health and protect the organ. While organ transplantation is certainly a medical miracle, much work remains to reduce rejection rates and move this therapy to a lifelong cure.
____
Trends in organ donation:
Since the start of transplantation, there has been a shortfall in the number of suitable donor organs available, and as the numbers of patients on the waiting lists has progressively increased, so too has the number of patients who are denied access to the waiting lists. At the end of March 2010, there were almost 8000 patients on the national waiting lists for an organ transplant in the UK, with more than 7000 waiting for a kidney or combined kidney and pancreas, 360 a liver, 254 a lung, and 144 a heart or heart and lungs. Patients are generally considered for listing for a transplant if they have a better than 50% chance of surviving 5 year after transplant, although the actual recipient survival after transplantation of all organ-types transplants is far better than this. Greater availability of suitable donor organs would allow these arbitrary thresholds to be relaxed.
Death while awaiting a transplant:
A significant number of patients fortunate enough to be on the transplant waiting list will die or be removed from the list at a later date, usually because they become too unfit for transplantation. Hence while 62% of patients awaiting a heart will be transplanted within a year, 12% will die and a further 7% will be removed from the waiting list in the same year. The situation is worse for lungs where 27% of patients will either die or be removed from the waiting list in the first year of listing, while only 31% will be transplanted; only a half of those patients listed for a lung transplant will ever be transplanted.
____
If I donate an organ, will I have health problems in the future?
Not necessarily. There are some organs you can give up all or part of without having long-term health issues. You can donate a whole kidney, or part of the pancreas, intestine, liver, or lung. Your body will compensate for the missing organ or organ part. If it is determined that donating an organ would put your health at risk in the short term or long term, then you would not be able to donate.
_
Some people have three or four kidneys.
Kidneys from deceased donors last for a median of nine years, and kidneys from living donors last for a median of 15 years (although some last much longer). For that reason, some people with kidney disease need more than one transplant in the course of their lives. These people can end up with three or four kidneys in their bodies because doctors usually don’t take the old organs out. (While these organs don’t work, they generally don’t cause any harm or discomfort, either.)
_
It’s possible to get more than one new organ.
Some people need more than one new organ at the same time — a heart and lungs, for example, or a kidney and a pancreas. Others need different organs at different times in their lives. For these groups, surgeons can sometimes transplant different organs at once or over time.
_
Transplantation not only saves lives, it improves quality of life:
Patients who receive organ transplants are statistically likely to live longer than those who need a transplant but opt for other types of care. For example, patients who are eligible and receive a kidney transplant are likely to live longer than those who remain on dialysis — and have a higher quality of life because they have fewer restrictions on their daily activities.
____
____
Opt-in versus opt-out system of organ donation:
As medical science advances, the number of people who could be helped by organ donors increases continuously. As opportunities to save lives increase with new technologies and procedures, the number of people willing to donate organs needs to increase as well. In order to respect individual autonomy, voluntary consent must be determined for the individual’s disposition of their remains following death. There are two main methods for determining voluntary consent: “opt in” (only those who have given explicit consent are donors) and “opt out” (anyone who has not refused consent to donate is a donor). In terms of an opt-out or presumed consent system, it is assumed that individuals do intend to donate their organs to medical use when they expire. Opt-out legislative systems dramatically increase effective rates of consent for donation as a consequence of the default effect. For example, Germany, which uses an opt-in system, has an organ donation consent rate of 12% among its population, while Austria, a country with a very similar culture and economic development, but which uses an opt-out system, has a consent rate of 99.98%.
_
Opt-out consent, otherwise known as “deemed” consent, support refers to the notion that the majority of people support organ donation, but only a small percentage of the population are actually registered, because they fail to go through the actual step of registration, even if they want to donate their organs at the time of death. This could be resolved with an opt-out system, where many more people would be registered as donors when only those who object consent to donation have to register to be on the non-donation list. For this reasons, countries, such as Wales, have adopted a “soft opt-out” consent, meaning if a citizen has not clearly made a decision to register, then they will be treated as a registered citizen and participate in the organ donation process. Likewise, opt-in consent refers to the consent process of only those who are registered to participate in organ donation. Currently, the United States has an opt-in system, but studies show that countries with an opt-out system save more lives due to more availability of donated organs. The current opt-in consent policy assumes that individuals are not willing to become organ donors at the time of their death, unless they have documented otherwise through organ donation registration. Registering to become an organ donor heavily depends on the attitude of the individual; those with a positive outlook might feel a sense of altruism towards organ donation, while others may have a more negative perspective, such as not trusting doctors to work as hard to save the lives of registered organ donors. Some common concerns regarding a presumed consent (“opt-out”) system are sociologic fears of a new system, moral objection, sentimentality, and worries of the management of the objection registry for those who do decide to opt-out of donation. Additional concerns exist with views of compromising the freedom of choice to donate and conflicts with religious beliefs which exist. Even though concerns exist, the United States still has a 95 percent organ donation approval rate. This level of nationwide acceptance may foster an environment where moving to a policy of presumed consent may help solve some of the organ shortage problem, where individuals are assumed to be willing organ donors unless they document a desire to “opt-out”, which must be respected. Because of public policies, cultural, infrastructural and other factors, presumed consent or opt-out models do not always translate directly into increased effective rates of donation.
_
Presently three major legal frameworks govern the donation of organs worldwide. The UK, along with a number of European countries, e.g. Germany and Italy, and Canada, Australia, and New Zealand have ‘opting-in’ systems. This means that the person in lawful possession of the body may authorize the removal of organs and tissues. In practice donation is usually requested from the next-of-kin of the deceased. Many other countries, including e.g. Austria, Belgium, Spain and Singapore, have introduced ‘opt-out’ or ‘presumed consent’ systems that assume individuals have granted permission for their organs to be donated, unless they specify otherwise, in advance of their death. ‘Required request’ or routine enquiry of the next-of-kin of a potential donor, forms part of state law in the US. It provides for hospitals that fail to adopt ‘required request’ polices to be denied support from healthcare funding agencies.
________
________
WHO Guiding Principles on Human Cell, Tissue and Organ Transplantation:
In 1987 the fortieth World Health Assembly, concerned at the trade for profit in human organs, initiated the preparation of the first WHO Guiding Principles on Transplantation, endorsed by the Assembly in 1991 in resolution WHA44.25. These Guiding Principles have greatly influenced professional codes and practices as well as legislation around the world during almost two decades. After a consultation process that took several years, the Sixty-third World Health Assembly adopted resolution WHA63.22 on 21 May 2010, endorsing the updated WHO Guiding Principles and identifying areas of progress to optimize donation and transplantation practices.
_
Director-General’s report to the seventy-ninth session of the Executive Board pointed out that human organ transplantation began with a series of experimental studies at the beginning of this century. That report drew attention to some of the major clinical and scientific advances in the field since Alexis Carrel was awarded the Nobel Prize in 1912 for his pioneering work. Surgical transplantation of human organs from deceased, as well as living donors to sick and dying patients began after the Second World War. Over the past 30 years, organ transplantation has become a worldwide practice and has saved many thousands of lives. It has also improved the quality of life of countless other persons. Continuous improvements in medical technology, particularly in relation to tissue “rejection”, have brought about expansion of the practice and an increase in the demand for organs. A feature of organ transplantation since its commencement has been the shortage of available organs. Supply has never satisfied demand, and this has led to the continuous development in many countries of procedures and systems to increase supply. Rational argument can be made to the effect that shortage has led to the rise of commercial traffic in human organs, particularly from living donors who are unrelated to recipients. There is clear evidence of such traffic in recent years, and fears have arisen of the possibility of related traffic in human beings. Health Assembly resolutions WHA40.13 and WHA42.5 are an expression of international concern over these developments.
_
These Guiding Principles are intended to provide an orderly, ethical, and acceptable framework for regulating the acquisition and transplantation of human organs for therapeutic purposes. The term “human organ” is understood to include organs and tissues but does not relate to human reproduction, and accordingly does not extend to reproductive tissues, namely ova, sperm, ovaries, testicles or embryos, nor is it intended to deal with blood or blood constituents for transfusion purposes. The Guiding Principles prohibit giving and receiving money, as well as any other commercial dealing in this field, but do not affect payment of expenditures incurred in organ recovery, preservation and supply. Of particular concern to WHO is the protection of minors and other vulnerable persons from coercion and improper inducement to donate organs. Organs and tissues (referred to in this text as “organs”) may be removed from the bodies of deceased and living persons for the purpose of transplantation only in accordance with the following Guiding Principles.
_
WHO Guiding Principles on Human Cell, Tissue & Organ Transplantation 2010:
| 1 | Cells, tissues, and organs may be removed from the bodies of deceased persons for the purpose of transplantation if: any consent required by law is obtained, and there is no reason to believe that the deceased person objected to such removal |
| 2 | Physicians determining that a potential donor has died should not be directly involved in cell, tissue, or organ removal from the donor or subsequent transplantation procedures; nor should they be responsible for the care of any intended recipient of such cells, tissues, and organs |
| 3 | Donation from deceased persons should be developed to its maximum therapeutic potential, but adult living persons may donate organs as permitted by domestic regulations. In general, living donors should be genetically, legally, or emotionally related to their recipients. Live donations are acceptable when the donor’s informed and voluntary consent is obtained, when professional care of donors is ensured and follow-up is well organized, and when selection criteria for donors are scrupulously applied and monitored. Live donors should be informed of the probable risks, benefits, and consequences of donation in a complete and understandable fashion; they should be legally competent and capable of weighing the information; and they should be acting willingly, free of any undue influence or coercion |
| 4 | No cells, tissues, or organs should be removed from the body of a living minor for the purpose of transplantation other than narrow exceptions allowed under national law. |
| Specific measures should be in place to protect the minor and, wherever possible, the minor’s assent should be obtained before donation. What is applicable to minors also applies to any legally incompetent person | |
| 5 | Cells, tissues, and organs should only be donated freely, without any monetary payment or other reward of monetary value. Purchasing, or offering to purchase, cells, tissues, or organs for transplantation, or their sale by living persons or by the next of kin for deceased persons, should be banned. The prohibition on sale or purchase of cells, tissues, and organs does not preclude reimbursing reasonable and verifiable expenses incurred by the donor, including loss of income, or paying the costs of recovering, processing, preserving, and supplying human cells, tissues, or organs for transplantation |
| 6 | Promotion of altruistic donation of human cells, tissues, or organs by means of advertisement or public appeal may be undertaken in accordance with domestic regulation. Advertising the need for or availability of cells, tissues, or organs, with a view to offering or seeking payment to individuals for their cells, tissues, or organs, or, to the next of kin, where the individual is deceased, should be prohibited. Brokering that involves payment to such individuals or to third parties should also be prohibited |
| 7 | Physicians and other health professionals should not engage in transplantation procedures, and health insurers and other payers should not cover such procedures, if the cells, tissues, or organs concerned have been obtained through exploitation or coercion of, or payment to, the donor or the next of kin of a deceased donor |
| 8 | All health-care facilities and professionals involved in cell, tissue, or organ procurement and transplantation procedures should be prohibited from receiving any payment that exceeds the justifiable fee for the services rendered |
| 9 | The allocation of organs, cells, and tissues should be guided by clinical criteria and ethical norms, not financial or other considerations. Allocation rules, defined by appropriately constituted committees, should be equitable, externally justified, and transparent |
| 10 | High-quality, safe, and efficacious procedures are essential for donors and recipients alike. The long-term outcomes of cell, tissue, and organ donation and transplantation should be assessed for the living donor and the recipient in order to document benefit and harm. The level of safety, efficacy, and quality of human cells, tissues, and organs for transplantation, as health products of an exceptional nature, must be maintained and optimized on an ongoing basis. This requires implementation of quality systems including traceability and vigilance, with adverse events and reactions reported, both nationally and for exported human products |
| 11 | The organization and execution of donation and transplantation activities, and their clinical results, must be transparent and open to scrutiny, while ensuring that the personal anonymity and privacy of donors and recipients are always protected |
_____
_____
Public policy:
The fields of solid organ and vascular composite allograft transplantation are dependent on the availability of donor organs. The transplant candidate waiting list in the United States continues to grow. The American Society of Transplantation (AST) recognizes the decision to donate organ(s) or a portion of an organ, as a truly selfless act, focused on the potential to save the life of another. Moreover, this decision may come at a particularly difficult time (impending death) for family members of a loved one. The AST supports the promotion and development of organ donor registries, and encourages the public to talk to their physicians and loved ones about end of life issues. The AST encourages its membership to sign up to be an organ donor by signing their organ donor card or by whatever means their state identifies them as an organ donor.
A number of strategies have been implemented to increase the number of organs donated; AST supports these efforts, which include:
- timely referral,
- routine notification and mandated choice,
- donation after circulatory determination of death,
- computerized donor registries and first person consent donor designation, and
- efforts to increase organ donation (such as the previous organ donation and transplantation breakthrough collaborative).
_
The United Kingdom has several different laws and policies for the organ donation process, such as consent of a witness or guardian must be provided to participate in organ donation. This policy is currently being consulted on by Department of Health and Social Care. In terms of effective organ donations, in some systems like Australia (14.9 donors per million, 337 donors in 2011), family members are required to give consent or refusal, or may veto a potential recovery even if the donor has consented. Some countries with an opt-out system like Spain (36 effective donors per million inhabitants) or Austria (21 donors/million) have high donor rates and some countries with opt-in systems like Germany (16 donors/million) or Greece (6 donors/million) have lower effective donation rates. The president of the Spanish National Transplant Organisation has acknowledged Spain’s legislative approach is likely not the primary reason for the country’s success in increasing the donor rates, starting in the 1990s. Looking to the example of Spain, which has successfully adopted the presumed consent donation system, intensive care units (ICUs) must be equipped with enough doctors to maximize the recognition of potential donors and maintain organs while families are consulted for donation. The characteristic that enables the Spanish presumed consent model to be successful is the resource of transplant coordinators; it is recommended to have at least one at each hospital where opt-out donation is practiced to authorize organ procurement efficiently.
_
Public views are crucial to the success of opt-out or presumed consent donation systems. In a study done to determine if health policy change to a presumed consent or opt-out system would help to increase donors, an increase of 20 to 30 percent was seen among countries who changed their policies from some type of opt-in system to an opt-out system. Of course, this increase must have a great deal to do with the health policy change, but also may be influenced by other factors that could have impacted donor increases.
_
Transplant Priority for Willing Donors is a newer method and the first to incorporate a ‘non-medical’ criteria into the priority system to encourage higher donation rates in the opt-in system. Initially implemented in Israel, it allows an individual in need of an organ to move up the recipient list. Moving up the list is contingent on the individual opting-in prior to their need for an organ donation. The policy applies nonmedical criteria when allowing the individual who has previously registered as an organ donor, or family has previously donated an organ, priority over another possible recipient. It must be determined that both recipients have identical medical needs prior to moving a recipient up the list. While incentives like this in the opt-in system do help raise donation rates, they are not as successful in doing so as the opt-out, presumed consent default policies for donation.
_
The Organ Donation Day is celebrated every year at August 13th, provides a great opportunity in everyone’s life to come ahead and pledge to donate their precious organs.
Objectives of organ donation day:
- To make aware people about the need of organ donation.
- To distribute the messages of organ donation all over the world.
- To remove the hesitations of the people about donating organs.
- To say a grateful thanks to the donors of organs.
- To motivate and encourage more people towards organ donation in their life.
______
______
Brief History of organ donation and transplantation:
The first reasonable account is of the Indian surgeon Sushruta in the 6th century BC, who used autografted skin transplantation in nose reconstruction, a rhinoplasty. Success or failure of these procedures is not well documented. Centuries later, the Italian surgeon Gasparo Tagliacozzi performed successful skin autografts; he also failed consistently with allografts, offering the first suggestion of rejection centuries before that mechanism could possibly be understood. He attributed it to the “force and power of individuality” in his 1596 work De Curtorum Chirurgia per Insitionem.
_
The first successful corneal allograft transplant was performed in 1837 in a gazelle model; the first successful human corneal transplant, a keratoplastic operation, was performed by Eduard Zirm at Olomouc Eye Clinic, now Czech Republic, in 1905. The first transplant in the modern sense – the implantation of organ tissue in order to replace an organ function – was a thyroid transplant in 1883. It was performed by the Swiss surgeon and later Nobel laureate Theodor Kocher. In the preceding decades Kocher had perfected the removal of excess thyroid tissue in cases of goiter to an extent that he was able to remove the whole organ without the person dying from the operation. Kocher carried out the total removal of the organ in some cases as a measure to prevent recurrent goiter. By 1883, the surgeon noticed that the complete removal of the organ leads to a complex of particular symptoms that we today have learned to associate with a lack of thyroid hormone. Kocher reversed these symptoms by implanting thyroid tissue to these people and thus performed the first organ transplant. In the following years Kocher and other surgeons used thyroid transplantation also to treat thyroid deficiency that appeared spontaneously, without a preceding organ removal. Thyroid transplantation became the model for a whole new therapeutic strategy: organ transplantation. After the example of the thyroid, other organs were transplanted in the decades around 1900. Some of these transplants were done in animals for purposes of research, where organ removal and transplantation became a successful strategy of investigating the function of organs. Kocher was awarded his Nobel Prize in 1909 for the discovery of the function of the thyroid gland. At the same time, organs were also transplanted for treating diseases in humans. The thyroid gland became the model for transplants of adrenal and parathyroid glands, pancreas, ovary, testicles and kidney. By 1900, the idea that one can successfully treat internal diseases by replacing a failed organ through transplantation had been generally accepted. Pioneering work in the surgical technique of transplantation was made in the early 1900s by the French surgeon Alexis Carrel, with Charles Guthrie, with the transplantation of arteries or veins. Their skilful anastomosis operations and the new suturing techniques laid the groundwork for later transplant surgery and won Carrel the 1912 Nobel Prize in Physiology or Medicine. From 1902, Carrel performed transplant experiments on dogs. Surgically successful in moving kidneys, hearts, and spleens, he was one of the first to identify the problem of rejection, which remained insurmountable for decades. The discovery of transplant immunity by the German surgeon Georg Schöne, various strategies of matching donor and recipient, and the use of different agents for immune suppression did not result in substantial improvement so that organ transplantation was largely abandoned after WWI. In the late 1940s Peter Medawar, working for the National Institute for Medical Research, improved the understanding of rejection. Identifying the immune reactions in 1951, Medawar suggested that immunosuppressive drugs could be used. Cortisone had been recently discovered and the more effective azathioprine was identified in 1959, but it was not until the discovery of cyclosporine in 1970 that transplant surgery found a sufficiently powerful immunosuppressive.
_
Timeline of transplants:
- 1823: First skin autograft-transplantation by Carl Bunger, who documented the first modern successful skin graft on a person. Bunger repaired a person’s nose destroyed by syphilis by grafting flesh from the inner thigh to the nose, in a method reminiscent of the Sushruta.
- 1905: First successful cornea transplant by Eduard Zirm (Czech Republic)
- 1908: First skin allograft-transplantation of skin from a donor to a recipient (Switzerland)
- 1950: First successful kidney transplant by Dr. Richard H. Lawler (Chicago, U.S.A.)
- 1954: First living related kidney transplant (identical twins) (U.S.A.)
- 1954: Brazil’s first successful corneal transplant, the first liver (Brazil)
- 1955: First heart valve allograft into descending aorta (Canada)
- 1963: First successful lung transplant by James D. Hardy with patient living 18 days (U.S.A.)
- 1964: James D. Hardy attempts heart transplant using chimpanzee heart (U.S.A)
- 1964: human patient lived nine months with chimpanzee kidneys, twelve other human patients only lived one to two months, Keith Reemtsma and team (New Orleans, U.S.A.)
- 1965: Australia’s first successful (living) kidney transplant (Queen Elizabeth Hospital, SA, Australia)
- 1966: First successful pancreas transplant by Richard Lillehei and William Kelly (Minnesota, U.S.A.)
- 1967: First successful liver transplant by Thomas Starzl (Denver, U.S.A.)
- 1967: First successful heart transplant by Christian Barnard (Cape Town, South Africa)
- 1981: First successful heart/lung transplant by Bruce Reitz (Stanford, U.S.A.)
- 1983: First successful lung lobe transplant by Joel Cooper at the Toronto General Hospital (Toronto, Canada)
- 1984: First successful double organ transplant by Thomas Starzl and Henry T. Bahnson (Pittsburgh, U.S.A.)
- 1986: First successful double-lung transplant (Ann Harrison) by Joel Cooper at the Toronto General Hospital (Toronto, Canada)
- 1995: First successful laparoscopic live-donor nephrectomy by Lloyd Ratner and Louis Kavoussi (Baltimore, U.S.A.)
- 1997: First successful allogeneic vascularized transplantation of a fresh and perfused human knee joint by Gunther O. Hofmann
- 1997: Illinois’ first living donor kidney-pancreas transplant and first robotic living donor pancreatectomy in the U.S.A. University of Illinois Medical Center
- 1998: First successful live-donor partial pancreas transplant by David Sutherland (Minnesota, U.S.A.)
- 1998: First successful hand transplant by Dr. Jean-Michel Dubernard (Lyon, France)
- 1998: United States’ first adult-to-adult living donor liver transplant University of Illinois Medical Center
- 1999: First successful tissue engineered bladder transplanted by Anthony Atala (Boston Children’s Hospital, U.S.A.)
- 2000: First robotic donor nephrectomy for a living-donor kidney transplant in the world University of Illinois Medical Center
- 2004: First liver and small bowel transplants from same living donor into same recipient in the world University of Illinois Medical Center
- 2005: First successful ovarian transplant by Dr. P. N. Mhatre (Wadia Hospital, Mumbai, India)
- 2005: First successful partial face transplant (France)
- 2005: First robotic hepatectomy in the United States University of Illinois Medical Center
- 2006: Illinois’ first paired donation for ABO incompatible kidney transplant University of Illinois Medical Center
- 2006: First jaw transplant to combine donor jaw with bone marrow from the patient, by Eric M. Genden (Mount Sinai Hospital, New York City, U.S.A.)
- 2006: First successful human penis transplant (later reversed after 15 days due to 44-year-old recipient’s wife’s psychological rejection) (Guangzhou, China)
- 2008: First successful complete full double arm transplant by Edgar Biemer, Christoph Höhnke and Manfred Stangl (Technical University of Munich, Germany)
- 2008: First baby born from transplanted ovary. The transplant was carried out by Dr Sherman Silber at the Infertility Centre of St Louis in Missouri. The donor is her twin sister.
- 2008: First transplant of a human windpipe using a patient’s own stem cells, by Paolo Macchiarini (Barcelona, Spain)
- 2008: First successful transplantation of near total area (80%) of face, (including palate, nose, cheeks, and eyelid) by Maria Siemionow (Cleveland Clinic, U.S.A.)
- 2009: Worlds’ first robotic kidney transplant in an obese patient University of Illinois Medical Center
- 2010: First full facial transplant by Dr. Joan Pere Barret and team (Hospital Universitari Vall d’Hebron on 26 July 2010, in Barcelona, Spain)
- 2011: First double leg transplant by Dr. Cavadas and team (Valencia’s Hospital, La Fe, Spain)
- 2012: First Robotic Alloparathyroid transplant. University of Illinois Chicago
- 2013: First successful entire face transplantation as an urgent life-saving surgery at Maria Skłodowska-Curie Institute of Oncology branch in Gliwice, Poland.
- 2014: First successful uterine transplant resulting in live birth (Sweden)
- 2014: First successful penis transplant. (South Africa)
- 2014: First neonatal organ transplant. (U.K.)
_
First Successful Kidney Transplant 1950:
Ruth Tucker, 49, suffered from polycystic kidneys and was in need of a new kidney. One of her kidneys was non-functioning and the other only functioned at 10 percent. Tucker’s mother and sister had also died from the same disease. The doctors, hospital leadership and patient bravely decided to attempt something that hadn’t been done before—an organ transplant. History was made at Little Company of Mary Hospital on June 17, 1950, when doctors performed the first successful organ transplant in the world.
![]()
Tucker had waited at the hospital for five weeks prior to June 17 for a suitable donor. That morning, a healthy kidney became available from a woman who had died of cirrhosis of the liver. A photographer who had been hired to take a motion picture of the procedure fainted midway through—apparently not used to seeing operations. Luckily, plenty of backup was at hand, as around 40 doctors looked on during the surgery, including some standing on tables in the back to get a view of this historic event. One of the doctors in the audience took over behind the camera. At 11:30 AM, the kidney was removed from the donor, and 45 minutes later the transplant was complete, blood flowing through the kidney and Tucker recovering from the surgery. The surgery was extremely courageous, given that it was done without anti-infection drugs, tissue typing and other advances that are now standard. A Newsweek article a week after the surgery was headlined, “Borrowed from the Dead”. The article stated, “Successful transplants have been made of bones, skin, nerves, tendons and eye corneas. But up to last week, no vital human organ had ever been moved from one person to another. Then, in a daring surgical feat, Dr. Richard M. Lawler of the Little Company of Mary Hospital, Chicago, removed a diseased kidney from Mrs. Ruth Tucker…The patient was ‘willing to gamble rather than lie back and wait for death,’ Dr. Lawler said.” A month later, Tucker was released from the hospital, a medical miracle. She lived five years before dying from a coronary occlusion following pneumonia.
______
______
Epidemiology and statistics of organ donation and transplantation:
For many years, information on donation and transplantation activity in European countries has been published in an annual Council of Europe Transplant Newsletter. Recently, this has been extended to include information from North and South America and Australasia. However, an even more extensive database is the Global Observatory on Donation and Transplantation, established in 2007 under the auspices of the WHO and the Spanish transplant organisation (ONT), which is expected to develop over time to include both activity and outcome data.
_
According to activity data reported to the Global Observatory on Donation and Transplantation (GODT) (World Health Organization 2012), analysis from 2010 transplant activity for 95 countries, representing nearly 90% of the worldwide population, shows that ∼106,879 solid organ transplants were performed worldwide: 73,179 kidney transplants (46% from living donors), 21,602 liver transplants (15% from living donors), 5582 heart transplants, 3927 lung transplants, 2362 pancreas transplants, and 227 small bowel. This activity increased 2.12% during 2009, but it is estimated that it is far from global needs. On the other hand, there are huge geographical differences on transplant activity ranging from >70 per million population (pmp) in developed countries to 0–2.4 pmp in developing countries. In 2014, 119,873 solid organ transplants were performed worldwide … Although impressive; the annual number of organ transplants represents less than 10% of the global needs. Organ shortage leads to deaths and poor quality of life for those on the waiting list.
_
Some estimates of the number of transplants performed in various regions of the world have been derived from the Global Burden of Disease Study.
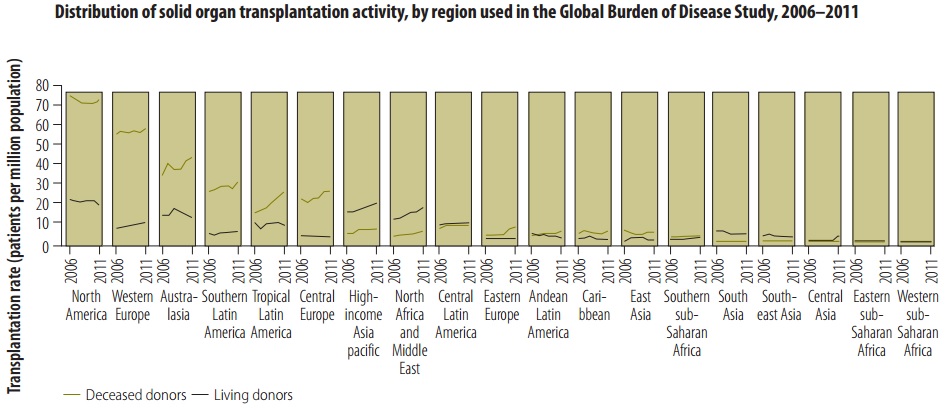
Figure above shows the distribution of solid organ transplantation activities across regions specified by the Global Burden of Disease study. Both living and deceased donor transplantation activity increased in North Africa and the Middle East between 2006 and 2011. These regional increases were driven predominantly – in the case of deceased donor transplantation – by activities in the Islamic Republic of Iran and Turkey, and – in the case of living donor transplantation – by activities in Jordan and Saudi Arabia. Turkey experienced large increases in transplantation activity following the establishment of its National Coordination Centre in 2001. The establishment of this centre brought Turkish organ procurement and transplantation under the control of the national Ministry of Health and reoriented donation and transplantation around hospital-based transplant coordinators. Similar reforms to systems for donor identification, management and organ recovery in the Republic of Korea were probably important contributors to the increases in transplantation activity also observed for the high-income Asia Pacific region between 2006 and 2011.
_
Organ donation and national income:
It is observed that, among transplanting countries, provision of deceased donor transplantation remains significantly associated with gross national income per capita. This reflects the extra resources and organization needed to support deceased donor transplantation, including the requirements for a waiting list and allocation system, an organ procurement programme, an on-call transplantation team and relevant intensive-care resources as seen in the figure below. For many low- and middle-income countries, the costs of post-transplantation care and on-going immunosuppression present a substantial additional barrier to the development of greater transplantation capacity.
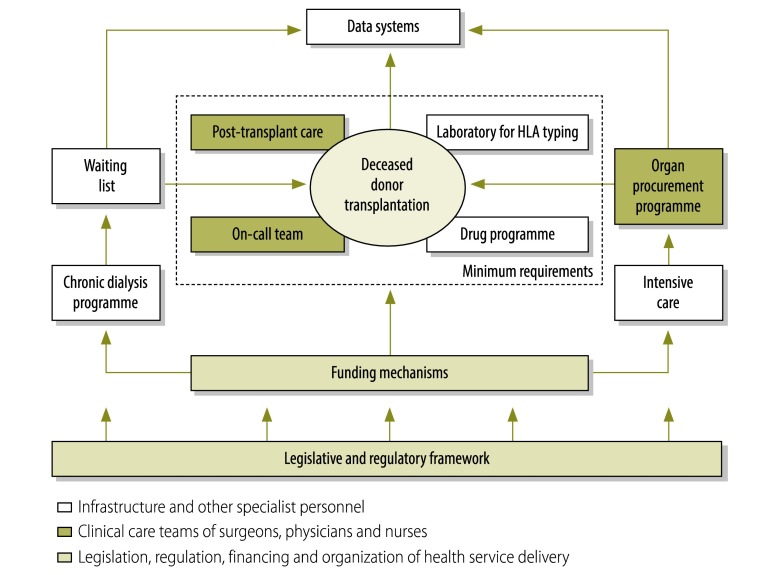
Figure above shows Schematic of the minimum health system requirements for performing deceased donor organ transplantation.
__
Important Organ Donation Statistics in April 2018:
In the United States alone:
- Someone is added to the organ donation waiting list every 10 minutes.
- Approximately 20 people die every day waiting for an organ.
- More than 114,845 people are waiting for an organ.
Statistics on Specific Organs:
If you’re interested in data relating to a specific type of organ donation, these statistics may interest you. The following numbers indicate the number of patients on the organ donation waiting list:
- Kidney: 95,095 people.
- Liver: 13,956 people.
- Heart: 3,987 people.
- Lung: 1,438 people.
- Pancreas: 890 people.
The most commonly transplanted tissue in the United States is the cornea. There are more than 40,000 corneal transplants completed every year.
In 2016, UNOS tallied a total of 33,598 completed organ transplants, up from 30,969 in 2015 and 29,535 in 2014. While these numbers are positively trending upwards, the fact remains that each day an average of 22 people die while waiting for a transplant. What’s most interesting is that one single person can potentially save the lives of more than eight others, if they are an organ — kidney, heart, lungs, pancreas, liver, intestine, and VCA — donor. And if someone is also a tissue donor — meaning they would donate bone, tendons, cartilage, connective tissue, skin, corneas, sclera, heart valves, and vessels — they can save, or change, the lives of nearly 75 people. But, according to Donate Life America, while 95 percent of U.S. adults support organ donation, only 54 percent are actual registered donors.
_
Some disturbing stats about ODT in India:
- Almost 175,000 people in India need a kidney; however, less than 5000 of them receive one.
- Only 1 out of 30 people who need a kidney receive one.
- 90% of people in the waiting list die without getting an organ.
- India’s annual liver transplant requirement is over100,000 but they manage only about 1000.
- 70% liver transplants are taken care of by a live donor, but only 30% are dependent on cadaver (deceased) donors.
- Annually more around 50000 hearts are required along with 20000 lungs.
Here are key reasons for the shortage of organ donors in India:
- Ignorance and Lack of Knowledge – There is a major lack of awareness about cadaveric organ transplant in India, and people would come forth if they received more information and ways to register for organ donation.
- Myths and Beliefs – The Indian society, mired in traditional beliefs, is not very amenable to the idea of cadaver organ transplants. What they fail to realize is that in a country with a long waiting list of transplants, they are spoiling the chance of someone leading a normal life, just because they want to consign the whole body to last rites.
- Expressing one’s wish to donate – Failure to record one’s wish about organ donation after death with a healthcare facility or with family members also is a major reason for the shortage of organs.
- India has an Opt-in system (consent for donation is required) as opposed to Opt-out system (implied consent), and the question of refusal of donation by the next of kin after brain death diagnosis is often the biggest hindrance in pushing this programme further.
_
At any given time, every major city in India would have 8–10 brain dead patients in various ICUs with 4–6% of all hospital deaths being brain death. In India, road accidents account for around 140,000 deaths annually and of these almost 65% sustain severe head injuries as per a study carried out by AIIMS, Delhi, meaning that there are almost 90,000 patients who may be brain dead. It is not that people do not want to donate, but that there are no mechanisms in hospitals to identify and certify brain deaths. It may also be pertinent to mention that no one empowers the relatives of a brain dead person to save lives of other people by donating their relative organs. Most importantly young deaths occurring either due to road traffic accidents or cardiovascular phenomenon provide the best option of yielding high quality organs but also requires air and road linkage (popularly known as dedicated green corridor) with appropriate trauma and transplant hospitals.
_
How is organ donation measured?
A number of factors are used to measure organ donation.
- Number of donors: this is a straight count of the number of organ donors.
- It is important to check if the donor count includes only deceased donors or also includes living donors (i.e. this occurs when a healthy person donates a kidney to someone in need and continues to live with just one kidney. It is also possible for a healthy person to donate part of his/her liver.).
- Deceased donors come from two pathways:
-Brain Dead (BD): irreversible cessation of all brain activity;
-Circulatory Death (CD): irreversible cessation of all circulatory and respiratory function.
- Donors Per Million Population (DPMP): this is a globally recognised measure that measures the number of donors per million people per year. This takes into account the differences in population size by country or state and enables a comparative measure to be made.
- When looking at the number of donors over a period of years it is important to adjust for population growth to see if numbers are growing in real terms. Tracking Donors per Million Population over time achieves this as the calculation already adjusts for population growth.
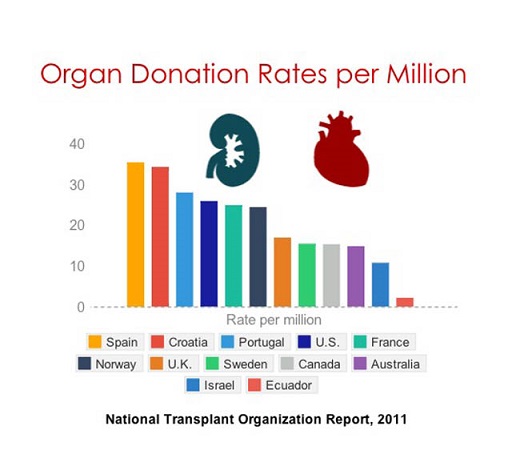
- In 2013, the leading countries in the world were Spain at 35.1 DPMP, Croatia at 35.0 DPMP and Malta at 34.0 DPMP. Australia was performing at 16.9 DPMP (16.1 DPMP in 2014).
- Number of transplant recipients: this is measure of the number of people who receive a transplant in a given period.
- When we divide the number of transplant recipients by the number of donors the number of transplants per donor is calculated. As at the end of 2014 the ratio is that for every one donor, 3.0 people receive a transplant.
_
Spanish organ donation rate highest in the world, demonstrating strategies for success:
The Organización Nacional de Trasplantes (ONT) created a model of coordination that enabled Spain to achieve the world’s highest rate of deceased organ donation at 40 donors per million population per year, according to an article published in the American Journal of Transplantation in 2017. In less than a decade, Spain increased from 15 donors per million population to 40 donors per million population through the ONT model. The Spanish model relies on health care professionals, namely intensive care physicians, to emphasize the importance of organ donation when a patient dies under circumstances that allow for organ donation. The model prioritizes identifying donation opportunities in EDs and hospital wards, in addition to intensive care units. Circulatory death — when circulation, heartbeat and breathing stop, as opposed to brain death — is also a circumstance in which donation is considered under this model. The most important success is that the system has made organ donation be routinely considered when a patient dies, regardless of the circumstances of death. Professionals attending to these patients in Spain consider that, in caring for patients at the end of their lives, it is their duty to systematically explore their wishes with regards to donating organs upon their death.
Spain is the undisputed world leader in organ transplants:
On an average, Spain performs up to 13 transplants a day, which translates to more than 1 transplant every two hours. A total of 5,259 organ transplants were carried out in Spain during 2017, beating the record of 4,818 from the year before, according to data published by ONT recently. Of these, 3,269 were kidney, 1,247 were liver, 363 were lungs, 304 were hearts,70 were pancreas and eight were intestines. It means that Spain saw 46.9 individual donors per million people (DPMP) in 2017, an increase from 43.9 DPMP in 2016 and 39.7 DPMP in 2015, “much higher” than the EU average (19.6) and the US average (26.6) according to stats published by Spain’s Health Ministry. In contrast, India’s rate of organ donation is a dismal 0.34 donors per million population. Simply put, only 1 out of approximately 3 million people in India donates organs after death
Spain has the highest deceased donor rate but that does not translate into the highest transplantation rates because of their low rate of living transplantation and their poor rate of utilisation of deceased donor kidneys. Switzerland’s 100 percentage use of deceased donor kidneys is remarkable. Ten countries achieved over 90% usage which leaves the question about the countries that do not achieve 85% at a minimum. We have no information on the quality of the deceased donor organs – but we understand that kidneys are considered from the oldest of deceased donors.
_
Living donation:
Living donation makes a significant contribution to kidney (and to a lesser extent liver) transplantation programmes worldwide and carries a number of advantages. Transplantation becomes elective and can be scheduled to the time the patient needs the transplant. Furthermore, the outcomes are better than if a deceased donor organ is used. However, this is at a cost. The mortality rate for living kidney donors is ∼1:3–5000, while for living liver donors, it may be as high as 1:200 according to one study. Morbidity occurs in 10–15% of patients and there are the added social and possibly financial costs to the donor. Living donation also opens the opportunity to commercialization and trafficking. Different countries have resolved these issues in different ways, depending at least in part on the availability of deceased donation, and living donor rates vary widely. The Netherlands, Turkey, Norway, and the USA now carry out over 20 donations per million population (DPMP) living donor kidney transplants per year; in the UK, the figure is 15.9 DPMP, whereas in Spain and France, the rate is ∼5 DPMP.
_____
_____
Reasons for organ donation:
Donor kidneys come from two sources: deceased organ donors or living donors. Deceased donors are people who have suffered brain death after a head trauma or medical problem in the brain such as bleeding. The families of these patients make the generous decision to donate their organs. Patients who are on the transplant wait list are waiting for organs from deceased donors. It is not uncommon for patients to wait many years for a deceased donor kidney.
_
Living related donors:
Living related donors donate to family members or friends in whom they have an emotional investment. The risk of surgery is offset by the psychological benefit of not losing someone related to them, or not seeing them suffer the ill effects of waiting on a list.
_
Good Samaritan:
Good Samaritan or “altruistic” donation is giving a donation to someone not well-known to the donor. Some people choose to do this out of a need to donate. Some donate to the next person on the list; others use some method of choosing a recipient based on criteria important to them. Web sites are being developed that facilitate such donation. It has been featured in recent television journalism that over half of the members of the Jesus Christians, an Australian religious group, have donated kidneys in such a fashion.
_
Financial compensation:
Now monetary compensation for organ donors is being legalized in Australia, and strictly only in the case of kidney transplant in the case of Singapore (minimal reimbursement is offered in the case of other forms of organ harvesting by Singapore). Kidney disease organizations in both countries have expressed their support. In compensated donation, donors get money or other compensation in exchange for their organs. This practice is common in some parts of the world, whether legal or not, and is one of the many factors driving medical tourism. In the illegal black market the donors may not get sufficient after-operation care, the price of a kidney may be above $160,000, middlemen take most of the money, the operation is more dangerous to both the donor and receiver, and the receiver often gets hepatitis or HIV. In legal markets of Iran the price of a kidney is $2,000 to $4,000.
_
In the United States, The National Organ Transplant Act of 1984 made organ sales illegal. In the United Kingdom, the Human Organ Transplants Act 1989 first made organ sales illegal, and has been superseded by the Human Tissue Act 2004. In 2007, two major European conferences recommended against the sale of organs. Recent development of web sites and personal advertisements for organs among listed candidates has raised the stakes when it comes to the selling of organs, and have also sparked significant ethical debates over directed donation, “good-Samaritan” donation, and the current U.S. organ allocation policy. Bioethicist Jacob M. Appel has argued that organ solicitation on billboards and the internet may actually increase the overall supply of organs. Many countries have different approaches to organ donation such as: the opt-out approach and many advertisements of organ donors, encouraging people to donate. Although these laws have been implemented into a certain country they are not forced upon very one as it is an individual decision.
_
Forced donation:
There have been concerns that certain authorities are harvesting organs from people deem undesirable, such as prison populations. The World Medical Association stated that prisoners and other individuals in custody are not in a position to give consent freely, and therefore their organs must not be used for transplantation. According to the Chinese Deputy Minister of Health, Huang Jiefu, approximately 95% of all organs used for transplantation are from executed prisoners. The lack of public organ donation program in China is used as a justification for this practice. In July 2006, the Kilgour-Matas report stated, “the source of 41,500 transplants for the six year period 2000 to 2005 is unexplained” and “we believe that there has been and continues today to be large scale organ seizures from unwilling Falun Gong practitioners”. Investigative journalist Ethan Gutmann estimates 65,000 Falun Gong practitioners were killed for their organs from 2000 to 2008.
______
Why you should consider organ donation?
Each year, thousands of people die while waiting for a transplant, because no suitable donor can be found for them. The need for organ donors has never been greater. For people with certain serious or life-threatening illnesses, and those suffering from organ failure, organ or tissue transplantation could mean a second chance at life. Donation is free of charge and anonymous. Improved survival rates now mean that most organ or tissue recipients enjoy many years of high-quality life after their transplant. Some people see donation as a great gift to others. Some see it as a sensible, practical thing to do after death. Within few months after burial, the bacteria will eat all our organs except bones. It takes 10 to 12 years to decompose a human body to skeleton buried at a depth of 2 meter. Instead of feeding yourself to bacteria, why shouldn’t we donate organs to someone who lives?

Each year, the number of people on the waiting list continues to be much larger than both the number of donors and transplants, which grow slowly. More importantly, only 3 in 1000 people die in the way that allows for organ donation according to one study. Every day across the UK, around three people who could have benefited from a transplant die because there aren’t enough organ donors. And currently around 6,500 people are on the waiting list for a transplant. Yet, out of approximately half a million people who die each year across the UK, only around 1% (5,603) die in circumstances where their organs could be donated. With such small numbers of people dying in the right circumstances to become an organ donor and so many adults and children in need of a transplant, it is vital that no opportunity for someone to become a donor is missed.
_______
_______
How to donate:
Becoming an organ donor is easy. You can indicate that you want to be a donor in the following ways:
- Register with the National Donate Life Registry. This ensures that your donor registration travels with you, no matter where you live or move across the country. You can register online at RegisterMe.org. Or if you have an iPhone with iOS 10, you can register through the Health app. Registrations submitted via iPhone go directly to the National Donate Life Registry.
- Designate your choice on your driver’s license. Do this when you obtain or renew your license.
- Tell your family. Make sure your family knows your wishes regarding donation. It’s also very important to tell your family that you want to be a donor. Hospitals seek consent from the next of kin before removing organs, although this is not required if you’re registered with the National Donate Life Registry or have donor designation on your driver’s license or state ID card.
- You may include your wishes in your living will if you have one, but that might not be immediately available at the time of your death.
- If you have designated someone to make health care decisions for you if you become unable to do so, make sure that person knows that you want to be an organ donor.
_
How do I pledge my organs in India?
Organs can be pledged online with National Organ & Tissue Transplant Organisation (NOTTO), which comes under the Government’s Ministry of Health and Family Welfare. You can also register at Organ Retrieval Banking Organization (ORBO), AIIMS Hospital, or NGOs like the Mohan Foundation, ORGAN India, Gift Your Organ Foundation, etc.
_
How Organ Transplants Work in USA:
To be included on the national waiting list, a patient must first find a transplant team that will treat him or her. The transplant team, a group of surgeons, nurses and other health professionals at a hospital, evaluates the patient to decide whether he or she is a good candidate for transplantation. In addition to assessing the patient’s physical condition, the team will consider the patient’s attitude, psychological state and history of drug abuse, among other factors. Donated organs are a rare and precious commodity, so doctors don’t want to proceed unless they are confident that a patient is physically and mentally prepared for the procedure, as well as life after the procedure. For the most part, patients who are unwilling to give up unhealthy drugs, including cigarettes and alcohol in many situations, will be automatically disqualified. If the transplant team feels that a patient is a good candidate for transplant, they will contact the UNOS Organ Center in Richmond, VA, in order to put the patient on the national waiting list. The Organ Center operators record all relevant information about the patient, including his or her physical condition, blood type, tissue type and age. This information is entered into the national database.
_
When an organ becomes available (when an organ donor is pronounced brain dead at a hospital, typically), the local organ procurement organization (OPO) will gather all relevant information about the donor and enter this data into a program maintained by the UNOS Organ Center. Based on the criteria established by the UNOS board of directors, the program generates a ranked list of potential recipients. The criteria involves several factors, including the physical compatibility between the donor and the recipient, the health of the recipient and how long the recipient has been waiting for an organ. The purpose of the criteria is to choose a recipient who is a good match and stands a good chance of recovery, while also taking into account who has been “in line” longer. The OPO will immediately contact the transplant team of the first person on the list. The transplant team will note all of the donor’s information and make a decision whether or not to accept the organ. It may choose to decline the organ if it feels that the donor and potential recipient are not a close enough match or that the organ is unsatisfactory. For example, the donor may be much larger or older than the potential recipient, making the organ a bad fit, or the donor may have had health problems that could have damaged the organ. The transplant team might also decline the organ if the potential recipient is ill or otherwise unprepared for surgery. If the organ is declined, the OPO will move to the next name on the list. In most cases, the OPO will first look for potential recipients in the local area. If there are no matches in the local area, the OPO will extend the search to anyone in the UNOS region (there are 11 regions across the country). If there are still no matches, the OPO will offer the organ to the person who is ranked first on the national list. The intention is to minimize organ transportation time and to encourage donation by offering donors a chance to help out their local community.
______
______
Benefits of organ donation and transplantation:
Here I elaborate the benefits of the concept of donating the organs. Based on the understanding of the people, the pros will certainly outweigh the cons. But the bottom line is that the organ donation will help to improve the lives and certainly give the recipient a second chance to live. Some of the benefits of the organ donation are given below.
- Saving lives and improving quality of life:
It is possible for one organ donor to save up to 8 lives. More than 100,000 people just in the United States are waiting for an organ transplant right now. This includes critical organs, such as the heart, the liver, and the kidneys. When a person registers as an organ donor, it becomes possible to help save lives in ways that you may have never thought possible before. People who are waiting for an organ transplant are often dependent on costly treatments to survive. A person waiting for a kidney transplant, for example, may need to visit a dialysis clinic multiple times per week to have their blood cleaned. By being able to donate an organ, it becomes possible for that individual to return to a somewhat normal lifestyle that doesn’t have the same costly procedures that need to happen on a regular basis.
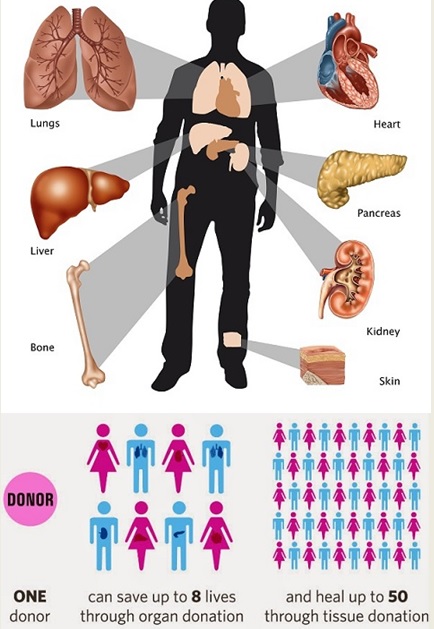
_
- It can offer a sense of closure:
For organ donations which occur out of tragedy, the process of organ donation can help families to find a sense of closure that wouldn’t happen otherwise. Knowing that the heart of a son, daughter, father, or mother continues to beat on in the chest of someone else can be a comforting experience. It won’t eliminate the grief that comes from losing a loved one, but it does communicate the idea that their loss is not in vain. Letting someone continue with their life is a gift that really does keep on giving. For the surviving relatives of a deceased donor, it gives a sense of goodness despite their loss and the tragedy they have experienced.
- For the living donor, it provides a good feeling and an opportunity to perform a humanitarian act, saving a complete stranger’s life with a portion of his liver, lung, intestine or pancreas.
- Transplantation is a highly cost effective treatment.
For example, to keep someone with renal failure alive costs an average of approximately $55,000-$80,000 per annum for kidney dialysis where a person can spend about 5 hours, 3 times a week having their blood ‘cleansed’. A kidney transplant costs around $40,000 for the first year and then up to $12,000 per year. Not only is a transplant more cost effective but it also provides a much better quality of life.
- It allows for the potential of medical research advances:
The concept of organ donation will help to enhance the medical research and scientific experiments. This will indirectly save the lives of the people. This has even allowed the scientists to comprehend the diseases and their effects they will have on the human body. The further advancement into the study of the organs with the help of the organ donation will help to find some treatments for the medical diseases that are still being considered. People can make donation to benefit science and medical research. This may include donating a specific organ, such as a heart or their brain. It can even include donating their entire body. For those who may have a rare disease or genetic condition, a donation such as this offers the potential of saving more lives through the knowledge gained.
___
Health-Related Quality of Life after Different Types of Solid Organ Transplantation, a 2000 study:
Outcomes after a procedure like transplantation have traditionally measured only operative and long-term survival and complication rates. Cost, quality of life (QOL), and return to work are gaining importance as outcome measures, especially because of the intense resource utilization that transplantation demands. Better technology and therapies have produced longer survival after transplantation, and attention is shifting to the quality of those life years. Quality of life is multidimensional. Health-related QOL can be divided into physical, psychological, and social domains of health. Each of these three components can be measured in two dimensions: objective assessment of functioning by clinical caregivers, and subjective perception of health by the patient and family members. The patient’s perspective is as important as that of the clinician. Measuring QOL means translating the various domains into quantitative values. Most tools measure QOL domains separately by clustering a few specific questions about each domain. Many tools are available that have been validated in various groups of patients and are applicable to a variety of health statuses, conditions, and diseases. In this study, authors applied three well-accepted tools to four different types of transplant patients with several goals: to describe functional health and health-related QOL before and after transplantation; to compare and contrast outcomes among liver, heart, lung, and kidney transplant patients; to compare these outcomes with selected norms; and to explore whether physiologic performance, demographics, and other clinical variables are predictors of posttransplantation overall subjective QOL. Different types of transplant patients have a different health-related QOL before transplantation. Performance improved after transplantation for all four types of transplants, but the trajectories were not the same. Subjective QOL also improved after transplantation. Path analysis shows the important predictors of health-related QOL. These data provide clearly defined and widely useful QOL outcome benchmarks for different types of solid organ transplants.
_____
Survival Benefit of Solid-Organ Transplant in the United States, a 2015 study:
Objective:
To determine the survival benefit of solid-organ transplant as recorded during a 25-year study period in the United Network for Organ Sharing (UNOS) database and the Social Security Administration Death Master File.
Design, Setting, and Participants:
In this retrospective analysis of UNOS data for solid-organ transplant during a 25-year period (September 1, 1987, through December 31, 2012), authors reviewed the records of 1,112,835 patients: 533,329 recipients who underwent a transplant and 579,506 patients who were placed on the waiting list but did not undergo a transplant.
Main Outcomes and Measures:
The primary outcome was patient death while on the waiting list or after transplant. Kaplan-Meier survival functions were used for time-to-event analysis.
Results:
Authors found that 2,270,859 life-years (2,150,200 life-years from the matched analysis) were saved to date during the 25 years of solid-organ transplant. A mean of 4.3 life-years were saved (observed to date) per solid-organ transplant recipient. Kidney transplant saved 1,372,969 life-years; liver transplant, 465,296 life-years; heart transplant, 269,715 life-years; lung transplant, 64,575 life-years; pancreas-kidney transplant, 79,198 life-years; pancreas transplant, 14,903 life-years; and intestine transplant, 4402 life-years.
Final analysis demonstrated that more than 2 million life-years were saved to date by solid-organ transplants during a 25-year study period. Transplants should be supported and organ donation encouraged.
In this study, authors documented the survival benefit of solid-organ transplants during a 25-year period (1987-2012)—a period that has seen unprecedented growth and improved outcomes in kidney, liver, heart, lung, pancreas, intestine, and combined organ transplants. Authors found that 2,270,859 life-years were saved in 533,329 patients through 2012. Because many of the transplant recipients in this study group are still alive, the number of life-years saved, thanks to this 25-year period of transplantation, will only increase until all the recipients in the cohort are deceased. This concept becomes readily apparent with the significant differences in the median survival time between patients on the waiting list and transplant recipients. This study included any patient who was ever listed for a solid-organ transplant from 1987 through 2012 (n = 1,112,835 patients): only 533,329 (47.9%) of them actually underwent a solid-organ transplant. This immense study illustrates the powerful potential of the UNOS database.
A kidney transplant is often thought to be merely a life-enhancing (rather than lifesaving) procedure in that recipients are simply relieved of the requirement of dialysis. However, as other studies have done in the past, this study clearly indicated that a kidney transplant is also a lifesaving procedure. The number of life-years saved per kidney transplant recipient is akin to the number of life-years saved per liver transplant recipient. This study also found a profound advantage for adult kidney transplant recipients of living-donor transplants compared with deceased-donor transplants. This advantage is evident in the Kaplan-Meier curves and in the median survival time (18.5 years with a living donor vs. 9.8 years with a deceased donor). However, the advantage is not so pronounced for paediatric kidney transplant recipients.
In the same vein, a pancreas transplant is also a lifesaving procedure. The perception persists that a pancreas transplant is simply a convenient insulin replacement therapy, despite much evidence in the literature to the contrary. This study found a significant survival advantage for all types of pancreas transplants, with the strongest advantage for simultaneous pancreas and kidney transplant recipients (4.7 life-years per recipient). A pancreas transplant alone, an often controversial option, confers a median survival time of 13.6 years (compared with 8 years in patients on the waiting list).
This study also reaffirms the lifesaving potential of a liver transplant. The use of liver retransplantation has often been questioned, but authors found a significant survival advantage (although diminished compared with a primary liver transplant).
The past 3 decades of heart transplantation have demonstrated a clear survival benefit for adult and pediatric heart transplants. Moreover, advances in the care of patients with heart failure, especially through the use of artificial devices, have gradually improved survival time in patients on the waiting list. Additional transplants also are useful, but their usefulness is diminished compared with primary transplants. Previous studies found a survival benefit for adult lung transplant recipients. In this study, authors reached a similar conclusion.
Final Conclusion:
The 2.3 million life-years saved (2.15 million after adjustment) to date is a stellar accomplishment. These life-years saved are in patients with end-organ failure, who are among the sickest patients.
________
________
Organ donation and its types:
Organ donation is the process of a person donating their organs for transplant. These are given to someone with damaged organs that need to be replaced. An organ transplant may save a person’s life, or significantly improve their health and quality of life. Most people waiting for a donated organ need to have a kidney, heart, lung or liver transplant. One donor can help several people because a single donor can donate a number of organs, including:
- kidneys
- liver
- heart
- lungs
- small bowel
- pancreas
Tissues that can be donated include:
- the cornea
- bone
- skin
- heart valves
- tendons
- cartilage
All donors have the choice of which organs and tissues they wish to donate. Ideally, the donor and recipient must have similar blood and tissue type. But the transplant is still possible, even if this is not the case. However, the recipient must be given special treatments to ensure that the body will not reject the new organ.
_
Anyone can register to be a donor:
Anyone can register as a donor: young, old, large or small, ill or healthy. Donation involves multiple organs and tissues, which means people who are ill or using medication can still say ‘yes’; if an illness or medication would render a particular organ unsuitable for donation, there will often still be others that could be good candidates for a transplant. You are never too old to donate either; there is always a chance that you can donate an organ or tissue, whatever your age. Anyone younger than 18 years old must present a parent or guardian consent.
Anyone with HIV, severe infection, and actively spreading cancer will be excluded, even when the condition is discovered after death or while a donor is still alive.
Here are some of the approximate ages for organ and tissue donation:
- People of all ages can be considered for liver and kidney donation.
- Eyes can be donated up to the age of 85 years
- Lungs up to 70 years
- Hearts up to 65 years
- Heart valves up to 60 years
- Pancreas up to 45 years of age
- Skin can be donated at any age
_
The chances of you needing an organ donation are much higher than the chances of being able to donate once you die. It is much more likely that you will need an organ donation at some point in your life than that you will be able to donate one yourself. It is only possible to donate an organ if you die in hospital. In most cases this occurs when a person is brain-dead following a cerebral haemorrhage or traffic accident. This means that they are legally dead, but artificial respiration can keep the organs supplied with oxygen-rich blood, allowing them to remain suitable for transplanting. The fact that organ donation is so often impossible is what makes it so important that as many people as possible register to become donors.
_
Types of donation:
There are two types of organ donation—deceased donation and living donation.
There are three different ways of donating an organ. These are known as:
- donation after brain stem death (deceased donation)
- donation after cardiac death (deceased donation)
- live organ donation (living donation)
_
Organ donors may be living or may have died of brain death or circulatory death. Most deceased donors are those who have been pronounced brain dead. Brain dead means the cessation of brain function, typically after receiving an injury (either traumatic or pathological) to the brain, or otherwise cutting off blood circulation to the brain (drowning, suffocation, etc.). Breathing is maintained via artificial sources, which, in turn, maintains heartbeat. Once brain death has been declared the person can be considered for organ donation. Criteria for brain death vary. Because less than 3% of all deaths in the U.S. are the result of brain death, the overwhelming majority of deaths are ineligible for organ donation, resulting in severe shortages. Organ donation is possible after cardiac death in some situations, primarily when the person is severely brain injured and not expected to survive without artificial breathing and mechanical support. Independent of any decision to donate, a person’s next-of-kin may decide to end artificial support. If the person is expected to expire within a short period of time after support is withdrawn, arrangements can be made to withdraw that support in an operating room to allow quick recovery of the organs after circulatory death has occurred.
_
Tissue may be recovered from donors who die of either brain or circulatory death. In general, tissues may be recovered from donors up to 24 hours past the cessation of heartbeat. In contrast to organs, most tissues (with the exception of corneas) can be preserved and stored for up to five years, meaning they can be “banked.” Also, more than 60 grafts may be obtained from a single tissue donor. Because of these three factors—the ability to recover from a non-heart beating donor, the ability to bank tissue, and the number of grafts available from each donor—tissue transplants are much more common than organ transplants. The American Association of Tissue Banks estimates that more than one million tissue transplants take place in the United States each year.
_____
_____
Living donor:
In living donors, the donor remains alive and donates a renewable tissue, cell, or fluid (e.g., blood, skin), or donates an organ or part of an organ in which the remaining organ can regenerate or take on the workload of the rest of the organ (primarily single kidney donation, partial donation of liver, lung lobe, small bowel). Regenerative medicine may one day allow for laboratory-grown organs, using person’s own cells via stem cells, or healthy cells extracted from the failing organs.
There are three types of living donors:
- Living related donors (LRD) are donors who are blood relatives of the recipient. Usually these are parents, children or siblings.
- Living unrelated donors (LURD) are not blood related and are usually spouses or friends of the recipient.
- A third type of living donor is called an altruistic donor or non-directed donor. These donors volunteer to donate a kidney to any person in need without knowledge of the recipient. In these cases, the transplant wait list or donor paired exchange can be used to select a recipient.
_
Directed donation:
This is a form of donation where a person donates an organ to a specific, identified recipient with whom they have a genetic or pre-existing emotional relationship for example parent to child, brother to sister or friend to friend.
Directed altruistic donation (DAD):
This is a form of donation where the organ is donated to a specific individual and there is no evidence of a qualifying genetic or pre-existing emotional relationship between the donor and recipient. These cases tend to be characterised by a third party – either a person or other mechanism such a social networking website – bringing the donor and recipient together for the purpose of transplantation, for example, a work colleague donating to a colleague’s child or an individual choosing to donate to a person they have seen in the local newspaper requiring a kidney.
Non-directed altruistic donation (NDAD):
This is a form of donation where a person donates an organ to an unknown recipient, that is, someone they have never met and that is not known to them. A non-directed altruistic donor donates into the paired/pooled scheme to create a ‘chain’ of transplants.
Non-directed altruistic donor chains:
This is a form of donation where a non-directed altruistic donor donates their organ into the paired/pooled scheme. Every three months transplant authority undertakes a matching run which matches pairs of donors and recipients together based on a range of factors. These include tissue type compatibility and blood group. By matching two or more donors and recipients, a chain of operations can be carried out. The remaining organ at the end of the chain is then donated to the best-matched recipient on the national waiting list.
_
Living donors potentially can donate:
- One of two kidneys
A kidney is the most frequently donated organ from a living donor. The donor’s remaining kidney provides the necessary function needed to remove waste from the body.
- One of two lobes of their liver.
Cells in the remaining lobe of the liver grow or regenerate until the liver is almost its original size. This re-growth of the liver occurs in a short period of time in both the donor and recipient.
- A lung or part of a lung, part of the pancreas, or part of the intestines.
Although these organs do not regenerate, both the donated portion of the organ and the portion remaining with the donor are fully functioning.
Living Tissue Donation:
Some of the tissues donated by living donors are:
- Skin, after certain surgeries such as an abdominoplasty
- Bone after knee and hip replacements
- Healthy cells from bone marrow and umbilical cord blood
- Amnion, donated after childbirth
- Blood, including white and red blood cells, platelets, and the serum that carries blood cells throughout the circulatory system.
A healthy body can easily replace some tissues such as blood or bone marrow. Both blood and bone marrow can even be donated more than once since they are regenerated and replaced by the body after donation.
_
Approximately one in three donations in the US, UK and Israel is now from a live donor. Potential donors are carefully evaluated, based on medical and psychological grounds. This ensures that the donor is fit for surgery and has no disease that could bring undue risk or likelihood of a poor outcome for either the donor or recipient. The psychological assessment is to ensure the donor gives informed consent and is not coerced. In countries where paying for organs is illegal, the authorities may also seek to ensure that a donation has not resulted from a financial transaction. The relationship the donor has to the recipient has evolved over the years. In the 1950s, the first successful living donor transplants were between identical twins. In the 1960s–1970s, live donors were genetically related to the recipient. However, during the 1980s–1990s, the donor pool was expanded further to emotionally related individuals (spouses, friends). Now the elasticity of the donor relationship has been stretched to include acquaintances and even strangers (‘altruistic donors’).
_
In carefully screened kidney donors, survival and the risk of end-stage renal disease appear to be similar to those in the general population. However, some more recent studies suggest that lifelong risk of chronic kidney disease is several-fold higher in kidney donors although the absolute risk is still very small. A 2017 article in the New England Journal of Medicine suggests that persons with only one kidney including those who have donated a kidney for transplantation should avoid high protein diet and limit their protein intake to less than one gram per kilogram body weight per day in order to reduce the long-term risk of chronic kidney disease. Women who have donated a kidney have a higher risk of gestational hypertension and preeclampsia than matched nondonors with similar indicators of baseline health. Traditionally, the donor procedure has been through a single incision of 4–7 inches (10–18 cm), but live donation is being increasingly performed by laparoscopic surgery. This reduces pain and accelerates recovery for the donor. Operative time and complications decreased significantly after a surgeon performed 150 cases. Live donor kidney grafts have higher long-term success rates than those from deceased donors. Since the increase in the use of laparoscopic surgery, the number of live donors has increased. Any advance which leads to a decrease in pain and scarring and swifter recovery has the potential to boost donor numbers. In January 2009, the first all-robotic kidney transplant was performed at Saint Barnabas Medical Center through a two-inch incision. In the following six months, the same team performed eight more robotic-assisted transplants. In 2009 at the Johns Hopkins Medical Center, a healthy kidney was removed through the donor’s vagina. Vaginal donations promise to speed recovery and reduce scarring. The recent advance of single port laparoscopy requiring only one entry point at the navel is another advance with potential for more frequent use.
____
____
Deceased donor:
Death can bring life is a unique concept new to mankind. The Egyptians were perhaps the first to believe in it and took elaborate measures to preserve the body by the complex process of embalming. In modern times, the field of preservation of tissues has constantly looked at newer methods of preserving tissues and organs after death. Preservation of cells is dependent on the complexity of their function. The more complex the function the lesser time the tissues can be preserved outside the body. Skin, bones, cartilage, arteries and veins are essentially structural tissues and have the ability to be preserved for many years whereas cells of organs like liver, heart, pancreas, lungs, kidneys, and intestine can only be preserved for few hrs to a few days. The concept of Brain Death is more recent and its acceptance as an entity has provided a boost to the whole organ donation and transplant programme in the world. In brain death patient it is possible to preserve the required hemodynamic stability to keep the critical organs alive by providing them with oxygen and nutrition. Organ donation in a brain death situation is a positive outcome of death which sometimes maybe unnecessary as it happens in road traffic accident. Over 50% of Brain Death involves young people with head injury due to a road traffic accident. The tragedy for the family members of the deceased at this unnecessary loss of life is immense. Organ donation is perhaps the only positive outcome of this grave tragedy provided the relatives agree to the process. However one must always remember that the condition was not invented for the benefit of organ donation and the wishes of the loved ones should always be respected and no pressure should be put on the relatives to donate. Ideally they should be aware of the concept in advance and should come themselves come forward for organ donation.
_
Deceased donors (formerly cadaveric) are people who have been declared brain-dead and whose organs are kept viable by ventilators or other mechanical mechanisms until they can be excised for transplantation. Apart from brain-stem dead donors, who have formed the majority of deceased donors for the last 20 years, there is increasing use of donation-after-circulatory-death-donors (formerly non-heart-beating donors) to increase the potential pool of donors as demand for transplants continues to grow. Prior to the recognition of brain death in the 1980s, all deceased organ donors had died of circulatory death. These organs have inferior outcomes to organs from a brain-dead donor. For instance, patients who underwent liver transplantation using donation-after-circulatory- death (DCD) allografts have been shown to have significantly lower graft survival than those from donation-after-brain-death (DBD) allografts due to biliary complications and PNF(primary non-function). However, given the scarcity of suitable organs and the number of people who die waiting, any potentially suitable organ must be considered.
_
Leading practice in organ donation:
Current leading practice in organ donation is a whole-of-hospital system to manage the deceased organ donation process. This system has been implemented within hospitals worldwide and has effectively increased the rate of deceased organ donations. Leading practice requires effective delivery of all actions in each step of the deceased organ donation process to achieve the optimal outcome. The process steps are:
- Donor detection
- Death declaration
- Donor and organ viability
- Donor maintenance
- Family interview
- Organ recovery
- Organ distribution
- Transplant
_
In order to be a deceased organ donor, a person needs to be in an intensive care unit (ICU) and on a ventilator (breathing machine). Donation is only considered after all life-saving methods to save a patient’s life have been tried.
Deceased donors can be divided in two groups:
- Donation after Brain-death (DBD) donors
Neurological determination of death (also referred to as ”brain death”) means the brain has permanently lost all function and a diagnosis of death using neurological criteria has been determined. Most organ donations are from brain stem dead donors. This means the donor has been confirmed brain stem dead following a severe brain injury. The circulation is supported by artificial ventilation until the donated organs have been removed. Heart-beating donations have a high success rate because the organs are supported by oxygenated blood until they are removed.
- Donation after Cardiac Death (DCD) donors
DCD is also known as donation after circulatory death or cardio-circulatory death.
Organs and tissue can also be donated after cardiac death. In these cases, the organs must be removed within a few minutes of the heart stopping to prevent them being damaged by a lack of oxygenated blood. Donation after Cardio-Circulatory Death (DCD) is an option for organ donation for patients with severe brain injuries once a decision has been made to remove all life-sustaining treatments. When a person’s heart permanently stops beating, they have experienced Cardio-Circulatory Death. DCD is still considered a relatively new technique. DCD has the potential to increase the number of available donor organs significantly. This technique is still poorly understood by many health-care professionals not directly involved in ODT and even more so by the general public, many of whom believe that organs are obtained solely from brain-dead patients (DBD).
_
The University of Wisconsin Organ and Tissue Donation service publishes the following as a guide describing the difference between organ donation after brain death (DBD) and organ donation after cardiac death (DCD).
| Donation After Brain Death (DBD) | Donation After Cardiac Death (DCD) | |
| Injury | Severe brain injury from trauma, cerebral vascular accident, anoxic event, other – REFERRAL TO OPO | Severe brain injury from trauma, cerebral vascular accident, anoxic event, other – REFERRAL TO OPO |
| Meets Criteria for Brain Death | Yes: Clinical Exam (including apnea test) is consistent with brain death. If unable to fully complete any part of the clinical exam, a confirmatory test is required (i.e., Nuclear Flow). | No: Some neurological reflex is still present |
| Prognosis | Brain death: This is the legal time of death | As determined by hospital physician, patient has no chance of recovery from brain injury; cannot survive without mechanical ventilator. |
| Action | Brain death declaration is made by hospital physician (not OPO).
Signed brain death note and consent form are faxed to OPO. Once brain death is declared, OPO and Hospital work cooperatively on medical management of the donor patient. Patient remains on ventilator throughout organ recovery.
Anesthesiology is present for intra-operative fluid and BP management Transplant team spends three to four hours recovering organs in-situ.
|
Family/NOK elects to withdraw support
Donation discussion with family, they consent. Signed futility note and consent form get faxed to OPO. OPO and hospital work cooperatively on medical management of the donor patient.
Withdrawal of support can take place in OR or ICU
Cardiac death
Wait five minutes to ensure no auto-resuscitation. After five minutes of ceased circulation, hospital physician (not OPO) declares death. Transplant team immediately begins organ recovery; takes one to two hours to recover organs en-bloc. |
| Potential organs | Heart, lungs, liver, pancreas, kidneys and intestine | Lungs, liver, pancreas and kidneys |
| Key Points | The time of brain death is legal time of death
Brain death is not a coma, it’s irreversible – brain cells do not recover
Organs dissected in-situ
Maintained on ventilator throughout the organ recovery |
DCD is only discussed with families after decision to withdraw support has been made
Rapid recovery of organs procured en-bloc
If patient doesn’t expire within two hours, organ donation is no longer possible, and the patient is returned to the sending unit. He/she is not re-intubated. RN to call OPO with CTOD. |
_
Brain death:
Brain death is irreversible cessation of cerebral and brain stem function characterized by the absence of electrical activity in the brain, blood flow to the brain, and brain function as determined by the clinical assessment of responses. A brain dead person is dead, although his or her cardiopulmonary functioning may be artificially maintained for some time. The American Association of Neurology (AAN) has defined brain death with three cardinal signs, cessation of the functions of the brain including the brainstem, coma or unresponsiveness and apnea. There is no global consensus in the criteria for establishing brain death, and significant differences exist in the tests used. Often caused by a severe injury or trauma, brain death is diagnosed through a series of clinically accepted tests including an apnea test that determines if a person can breathe while temporarily disconnected from the ventilator. Neurological death is permanent and cannot be reversed.
_
Although brain-dead (or “heart beating”) donors are considered to be dead, the donor’s heart continues to pump and maintain the circulation. This makes it possible for surgeons to start operating while the organs are still being perfused (supplied with blood). During the operation, the aorta will be cannulated, after which the donor’s blood will be replaced by an ice-cold storage solution, such as UW (Viaspan), HTK or Perfadex. Depending on which organs are transplanted, more than one solution may be used simultaneously. Due to the temperature of the solution, and since large amounts of cold NaCl-solution are poured over the organs for a rapid cooling, the heart will stop pumping. A brain-dead organ donor needs the same intensity of care with the focus of treatment directed toward organ perfusion and improved quality of grafts. Intensive care with the use of invasive lines is mandatory for improved quality of care and titration of inotropes and fluids. Adequate care for the donor targeting hemodynamic indices and lung protective ventilator strategies can improve graft quality for donation. Hormone supplementation using thyroxine, antidiuretic hormone, corticosteroid and insulin has shown to improve outcomes following transplant.
_
Organ recovery:
A beating heart cadaver is kept alive in order to keep its organs from decaying before they can be transplanted. Surgeons will remove the organs, one after the other, and have them transferred to the recipients’ treating teams. The entire recovery process is usually completed within four hours. This process was formerly known as an “organ harvest”, but the name has since changed to the milder “organ recovery”. Many organs can be extracted, and many lives can be saved by one body. Some donated organs are taken from non-heart-beating donors. Organs from brain deaths, however, have a better success rate, and currently most organ donation is from these deaths.
_____
Donation after circulatory death (DCD):
“Donation after Cardiac Death” donors are patients who do not meet the brain-dead criteria, but due to the unlikely chance of recovery, have elected via a living will or through family wishes, to have support withdrawn. In this procedure, treatment is discontinued (mechanical ventilation is shut off). After a time of death has been pronounced, the patient is rushed to the operating room, where the organs are recovered/removed. Storage solution is then flushed through the organs. Since the blood is no longer being circulated, coagulation must be prevented with large amounts of anti-coagulation agents such as heparin. Several ethical and procedural guidelines must be followed; most importantly, the organ recovery team should not participate in the patient’s care in any manner until after death has been officially declared. Patients in a coma are not considered for Donation after Cardio-Circulatory death since patients in a coma or vegetative state have varying levels of brain function and depending on the severity of the brain injury, these patients can live off of life support and can sometimes recover or wake up from a coma.
_
Donation after Circulatory Death (DCD), previously referred to as donation after cardiac death or non-heart beating organ donation, refers to the retrieval of organs for the purpose of transplantation from patients whose death is diagnosed and confirmed using cardio-respiratory criteria. There are two principal types of DCD, controlled and uncontrolled. Uncontrolled DCD refers to organ retrieval after a cardiac arrest that is unexpected and from which the patient cannot or should not be resuscitated. In contrast, controlled DCD takes place after death which follows the planned withdrawal of life-sustaining treatments that have been considered to be of no overall benefit to a critically ill patient on ICU or in the Emergency Department. The clinical circumstances in which DCD can occur are described by the Maastricht classification.
_
Donation after circulatory death (DCD) describes the retrieval of organs for the purposes of transplantation that follows death confirmed using circulatory criteria. The persisting shortfall in the availability of organs for transplantation has prompted many countries to re-introduce DCD schemes not only for kidney retrieval but increasingly for other organs with a lower tolerance for warm ischaemia such as the liver, pancreas, and lungs. DCD contrasts in many important respects to the current standard model for deceased donation, namely donation after brain death. The challenge in the practice of DCD includes how to identify patients as suitable potential DCD donors, how to support and maintain the trust of bereaved families, and how to manage the consequences of warm ischaemia in a fashion that is professionally, ethically, and legally acceptable. Many of the concerns about the practice of both controlled and uncontrolled DCD are being addressed by increasing professional consensus on the ethical and legal justification for many of the interventions necessary to facilitate DCD.
_
The modified Maastricht classification is widely used to categorize DCD (Table below). Categories I, II, and V describe organ retrieval that follows unexpected and irreversible cardiac arrest (uncontrolled DCD), while categories III and IV refer to retrieval that follows death resulting from the planned withdrawal of life-sustaining cardiorespiratory support (controlled DCD). It follows that uncontrolled DCD can only occur in centres where facilities for organ perfusion and retrieval are at immediate hand (i.e. close to or within a transplantation centre), whereas almost any intensive care unit (ICU) or emergency department (ED) should be able to support controlled DCD.
_
Modified Maastricht classification of DCD and the locations where mainly practiced.
| Category | Description | Type of DCD | Locations practiced |
| I | Dead on arrival | Uncontrolled | ED in a transplant centre |
| II | Unsuccessful resuscitation | Uncontrolled | ED in a transplant centre |
| III | Anticipated cardiac arrest | Controlled | ICU and ED |
| IV | Cardiac arrest in a brain-dead donor | Controlled | ICU and ED |
| V | Unexpected arrest in ICU patient | Uncontrolled | ICU in a transplant centre |
ICU, intensive care unit; ED, emergency department
_____
Synopsis of types of organ donation:
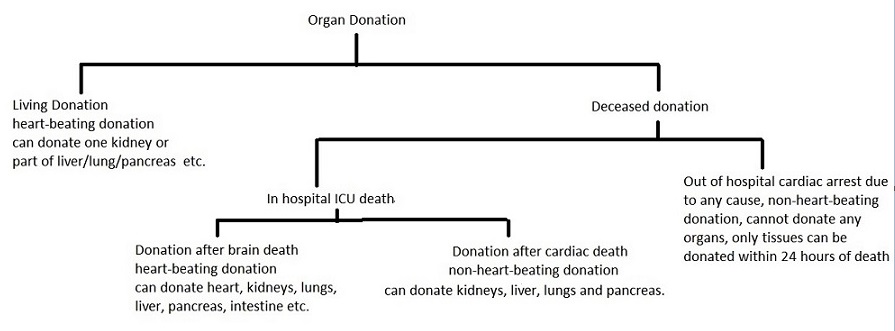
Solid organ donation (kidney, heart, lungs, liver, pancreas and intestine) requires blood circulation to be maintained in these organs until retrieval. This is possible only in brain death where the functioning of these organs can be supported for some time.
_____
Dead donor rule (DDR):
Currently, organs for transplant are recovered after determination of the donor’s death. This standard practice, commonly known as the “dead donor rule”, requires that the intended donor be declared dead before the removal of any life-sustaining organs. This rule was introduced to protect the person’s life before death and to prevent that lives were ended for the purpose of procuring organs. This rule is important to maintain the public trust in organ donation and transplantation and to avoid the misconception that care is withdrawn from potential donors in order to expedite death for the purpose of organ recovery.
_
Does DCD satisfy dead donor rule?
A 45 year old female patient arrives in the emergency department after having complained of a headache and progresses to unresponsiveness. She is placed on mechanical ventilation and a CT scan of her brain shows massive intracranial bleed. The family is assured she will probably progress to brain death but she doesn’t. After two days in the intensive care unit she continues with gasping ventilations and some flexion to pain in one arm. All other brain functions are absent. Her hemodynamics and other organ function are stable. The family desires the patient to be an organ donor but she is clearly not brain dead. It is suggested to the family that the patient can still donate under the ‘Donation after Cardiac Death’ (DCD) rules. Life support can be withdrawn and she can be pronounced dead using asystole as a criterion rather than brain death, following which organs can be taken for transplantation after a variable period of time to rule out ‘auto-resuscitation’.
Would you recommend this procedure?
The question that arises from this case is: Is the DCD donor truly dead at the moment of organ recovery?
The Uniform Determination of Death Act (UDDA) established that death could be declared by either the irreversible cessation of circulatory functions or the irreversible cessation of the entire brain, including the brain stem. DCD advocates cite this statute as evidence that DCD is a legitimate practice using the circulatory criterion.
The traditional concept of death is the irreversible cessation of the integrated functioning of the organism as a whole. It can be argued that DCD does not fulfil this definition. The New England Journal of Medicine states, “It is clear that a person is not dead until his brain is dead. The time honoured criteria of the stoppage of the heart beat and circulation are indicative of death only when they persist long enough for the brain to die.”
Organ donation operate under the dead donor rule (DDR), which stipulates that organs may not be removed prior to death nor may organ procurement cause or hasten death. DCD fails to satisfy the DDR on three counts in the above case: First, it manipulates the definition of irreversibility based on a moral position not to resuscitate; second, it appeals to fallacious logic that because one cannot auto-resuscitate then one is dead; and third, it focuses solely on the circulatory criterion which does not immediately correlate with brain status. Generally speaking, using the circulatory criterion would not be problematic as its absence will inevitably cause total brain failure. In DCD, however, the need for speed becomes a factor such that organs will be removed before the requisite time it takes for the brain to die as cessation of cardio-respiratory functions does not cause the brain to die immediately. If the body can be resuscitated, we have to question if it was ever really dead given our conventional notion of death as a finality from which one cannot be returned or resurrected from under any circumstances. DCD protocols remove organs from a donor who is not irreversibly dead; if the whole brain is not yet dead, the patient cannot be dead.
_
Recently, however, the dead donor rule has been reconsidered. In the opinion of some ethicists, while the “dead donor rule” assures patients, families and health professionals that a patient is dead before removing organs, therefore making organ transplantation legally and ethically acceptable, on the other hand it may jeopardize donation in selected cases. As an example, it is quoted the case of a DCD potential donor with prolonged agonal phase (the interval between withdrawal of support and cardiac arrest) that prevented organ recovery and transplantation due to prolonged ischemia. It is argued by some that, after the decision of withdrawing support has been reached, organs be procured without waiting for the declaration of death by circulatory criteria (i.e., cardiac arrest). The advantage of this pathway would be to give patients the opportunity to donate even before death is declared, when death is imminent (“near death”) and donation is desirable, in order not to jeopardize the viability of donated organs for transplant. It is argued that, when death is very near, some patients may want to die in the process of helping others to live, even if that means altering the timing or manner of their death. Regardless of this debate about the dead donor rule, it is important that ICU physicians, transplant professionals and organ procurement organizations make every effort towards maintaining public trust. Mistrust from the general public regarding the procurement of organs will likely result in reduced consent rates for donation based on the perceived fear by the donor’s family that treatment is withdrawn from their loved one in order to obtain organs. In other words, fearful people will assume that physicians care more about obtaining organs than saving the patient’s life. In addition, this debate on the dead donor rule emphasizes the importance of integration of organ donation with end-of-life care. By this integration, the donation process starts before the occurrence of the donor’s death, at the time when the potential donor with irreversible devastating brain injury is referred but is not yet declared dead. Since every actual donor has been a potential donor sometime before in the process, it is likely that the coordination of end-of-life care and organ donation would allow to identify and manage potential donors early in the process, increasing the chances of donation. The process leading from donation to transplantation can be described in the following 6 steps: Brain injury, referral, brain death, consent, organ recovery and organ transplantation (Figure below).
_
The process of deceased organ donation:
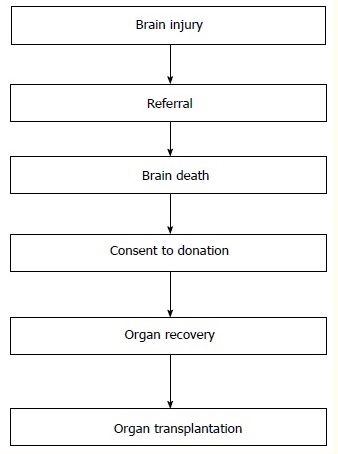
____
____
FAQ about organ donation:
- I have pledged to donate my organs, but that’s only possible in the event of brain death. What happens in the case of natural death?
Only tissues such as cornea, heart valves, skin, and bones can be donated. If a person dies naturally, the heart stops beating because of which the oxygen supply to the organs gets cut-off leaving them unfit for donation. Family members of the deceased person would have to contact the nearest eye or tissue bank in the case of natural death.
- Once I take the pledge, is organ donation legally binding?
The act of pledging only says that ‘I wish to donate my organs’, there is no legal binding to the pledge. Since organ donation isn’t legally binding, there’s not much paperwork involved.
- Does my family have to know about my decision to pledge my organs? Is the donor card not enough to convey my wish to donate my organs?
Yes, it is pertinent that family members know and agree with the individual’s decision to donate. The individual’s decision can be reversed by the family when the time comes. Since the final decision rests with the family, they must be informed about the decision to donate organs.
- I don’t need to donate because thousands of others do.
Few people die in such a way that donation is possible. Organ donors need to die in hospital where their body can be kept on a ventilator until the organs can be donated. In some cases, families do not give consent for donation to take place because they did not know the wishes of their deceased family member.
_____
Re-donation:
A few transplants out of the thousands performed every year involve the same organ spending time in more than two bodies. The most common scenario arises when a patient in the late stages of a disease receives a new liver or kidney as a last-ditch effort to keep him alive. If he dies shortly after, and the new organ wasn’t the cause, re-transplanting may be an option. There are a few good reasons, however, why donated organs aren’t often re-gifted. If the organ is coming from someone who was so sick that he needed a new organ, it probably lived a pretty rough second life. What’s more, dying involves the entire body shutting down. The trauma of dying can injure an organ. And then the second person dies, and the organ is taken out again. That’s more injury. But the main problem with the organ is the scar tissue that forms on it within weeks after the first surgery. That tissue must be removed before a second transplant, and doing so can injure the organ too much to make it worth re-donating. However, organs that are suitable for re-transplantation rarely spend much time in the first recipient, which means less time for scar tissue to form. So if you’re getting a third-hand kidney, chances are it’s almost as good as almost new.
_
Can an Organ Donor have an Autopsy?
Organ procurement for organ transplantation is a separate procedure that is performed by a surgical team in the operating room. Donating organs does not preclude the performance of an autopsy. In this case, the autopsy is performed in the autopsy suite after organs have been procured or removed by the surgical team. Of course, the organs which were removed for transplantation cannot be included in the autopsy examination. Sometimes the pathologist or medical examiner will attend the procedure or the operating surgeon will provide a report of findings for the doctor responsible for the autopsy.
_
Donation of the Entire Body:
If any donor donates his entire body, it will be used by the medical students to learn human anatomy and surgery in medical college. The benefit here is that the medical students can learn to become skilled in the art of saving others’ lives. This will certainly turn out to become an invaluable experience in their career.
_
Brain donation:
More people are suffering from brain diseases and disorders. There are no known cures for many of these conditions, and a high priority is given to research designed to improve our understanding of them, and find new treatments. To ensure research is thorough, it is also important to have access to brain tissues from people who did not have the diseases being studied. These unaffected tissues are known as ‘control tissues’. It is crucial that scientists have access to these so that they can be compared with tissues from people who had a disease. These valuable donations are essential for developing new and better treatments for people with diseases and in the search for a cure. Brain donation has helped researchers and doctors to better understand diseases such as schizophrenia, Alzheimer’s disease, Parkinson’s disease and variant Creutzfeldt-Jakob Disease. Potential brain donors are encouraged to contact their chosen brain bank rather than relying only on the information contained in their Will. By contacting the brain bank, appropriate arrangements can be discussed and made. This improves the chances of a successful donation after the person has died.
______
______
Organ transplantation and its types:
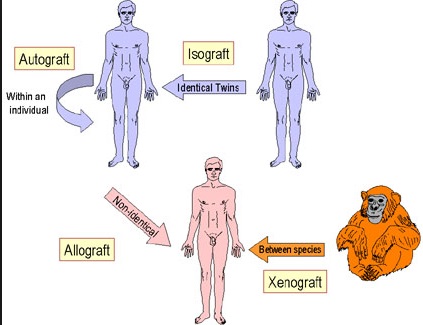
_
_
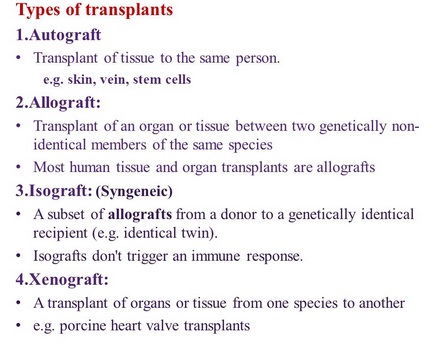
- Orthotopic graft- A graft placed in its normal anatomical site
- Heterotopic graft- A graft placed in a site different from its normal site
____
Types of transplant:
- Autograft:
A transplant from one part of your body to another part is called an autograft and the process is called autotransplantation. Autografts are the transplant of tissue to the same person. Sometimes this is done with surplus tissue, tissue that can regenerate, or tissues more desperately needed elsewhere (examples include skin grafts, vein extraction for CABG, etc.). Sometimes an autograft is done to remove the tissue and then treat it or the person before returning it (examples include stem cell autograft and storing blood in advance of surgery). In a rotationplasty, a distal joint is used to replace a more proximal one; typically a foot or ankle joint is used to replace a knee joint. The person’s foot is severed and reversed, the knee removed, and the tibia joined with the femur.
Some examples of autografts include:
- skin graft – uses healthy skin to help heal a wound or burn on another part of the body
- blood vessel graft – provides an alternative route for blood flow to bypass a blocked artery, for example, in heart bypass surgery
- bone graft – reconstructs a damaged area of the body, for example, in spinal fusion
- bone marrow graft – for example, in a person with cancer, bone marrow collected before chemotherapy can replace their blood stem cells after high-dose chemotherapy.
The advantage of an autograft is that the person’s body is unlikely to reject their own cells, so long-term medication to suppress the immune system (immunosuppressants) is not needed. However, the retrieval (collecting) of the tissue creates a new wound in addition to the transplant site, from which the person will need to recover.
- Allograft and allotransplantation:
An allograft is a transplant of an organ or tissue between two genetically non-identical members of the same species. The transplant is called an allograft, allogeneic transplant, or homograft. Most human tissue and organ transplants are allografts. Due to the genetic difference between the organ and the recipient, the recipient’s immune system will identify the organ as foreign and attempt to destroy it, causing transplant rejection.
- Isograft:
Isograft is a subset of allografts in which organs or tissues are transplanted from a donor to a genetically identical recipient (such as an identical twin). Isografts are differentiated from other types of transplants because while they are anatomically identical to allografts, they do not trigger an immune response. Monozygotic twins have the same major histocompatibility complex, leading to the low instances of tissue rejection by the adaptive immune system. Furthermore, there is virtually no incidence of graft-versus-host disease.
- Xenograft and xenotransplantation:
It is transplant of organs or tissue from one species to another. An example is porcine heart valve transplant, which is quite common and successful. Another example is attempted piscine-primate (fish to non-human primate) transplant of islet (i.e. pancreatic or insular tissue) tissue. The xenograft represents the most disparate of genetic relationships, because it is the transfer of tissue or organs between members of different species. Both allo-grafts and xenografts have the disadvantage that the recipient’s immune system is designed to recognize and reject foreign tissue.
- Domino transplants:
In people with cystic fibrosis (CF), where both lungs need to be replaced, it is a technically easier operation with a higher rate of success to replace both the heart and lungs of the recipient with those of the donor. As the recipient’s original heart is usually healthy, it can then be transplanted into a second recipient in need of a heart transplant, thus making the person with CF a living heart donor. This term is also used for a special form of liver transplant in which the recipient suffers from familial amyloidotic polyneuropathy, a disease where the liver slowly produces a protein that damages other organs. This patient’s liver can be transplanted into an older patient who is likely to die from other causes before a problem arises.
This term also refers to a series of living donor transplants in which one donor donates to the highest recipient on the waiting list and the transplant center utilizes that donation to facilitate multiple transplants. These other transplants are otherwise impossible due to blood type or antibody barriers to transplantation. The “Good Samaritan” kidney is transplanted into one of the other recipients, whose donor in turn donates his or her kidney to an unrelated recipient. Depending on the person on the waiting list, this has sometimes been repeated for up to six pairs, with the final donor donating to the person at the top of the list. This method allows all organ recipients to get a transplant even if their living donor is not a match to them. This further benefits people below any of these recipients on waiting lists, as they move closer to the top of the list for a deceased-donor organ.
- Split transplants:
Sometimes a deceased-donor organ, usually a liver, may be divided between two recipients, especially an adult and a child. This is not usually a preferred option because the transplantation of a whole organ is more successful.
____
Organ transplant process:
From living donations:
- The donor undergoes the medical tests and evaluations to check his or her medical compatibility with the recipient.
- The donor’s medical compatibility is confirmed by a doctor, only after which a transplant may take place.
- The donor’s organs are surgically retrieved and stored in special chemical solutions until transplantation is to occur.
- The donor’s body is surgically closed.
- The donor may have to stay under medical care for a few days after organ retrieval has occurred.
Living donors, however, may only donate a limited list of organs or tissue.
_
From decease donations:
- The donor, who is a victim of a fatal injury to the head, is declared brain dead by a board of medical experts.
- Consent from the donor’s family is obtained before the process of organ procurement is carried out. In the interim, the donor’s body is kept on a ventilator under special medical care, which ensures that his or her heart is still beating and organs are kept alive.
- A suitable recipient(s) for the organ(s) is identified off a waiting list and notified.
- The donor’s organs are surgically retrieved and stored in special chemical solutions until transplantation is to occur.
- The ventilator support is discontinued and the donor’s body is surgically closed and released to the family.
____
Time is of the essence in organ transplant:
Organ transplantation is a highly time-sensitive process mastered by teams of more than 10 medical professionals that includes surgeons, nurses, anesthesiologists, etc. Once a family has decided to give the gift of life, the complex process begins as one surgeon preps the recipient while another surgeon travels to the donor at another center to procure the organ. The transplant process is often a race against the clock and one of the biggest challenge is the coordination between hospitals in the organ transfer and delivery process. Timing of a transplant is determined by when the donor is identified and the ability to coordinate the transplant among centers, which typically occurs in the middle of the night. Surgeons are accustomed to performing transplants in the wee hours. Time constraints for transplants also vary depending on the type of organ. Kidneys and livers can last up to 24 hours and 10 hours respectively outside the body before being implanted, but for hearts, the team prefers to perform the transplant within five hours of the organ being secured, and usually no longer than seven. But one unique advantage to hearts is that they grow within the body, giving surgeons the ability to transplant a wider variety of hearts in patients. Hearts have a more limited time frame to be outside the body, but they are more flexible when matching donors and recipients by size and age. For example, a newborn’s heart can grow to the size of an adult heart once it’s transferred.
____
Waiting time:
Waiting times vary because each patient’s situation is unique. Some patients’ medical conditions are far more life-threatening or are advancing more rapidly than others’ conditions. Also, patients receiving medical treatments respond differently, and this may make it easier or more difficult to find matches.
Factors that can affect a transplant candidate’s waiting time include the following:
- blood type
- tissue type
- height and weight of the transplant candidate
- size of the donated organ
- medical urgency
- distance between the donor’s hospital and the candidate’s transplant hospital
- the number of donors in the local area
- the transplant program’s criteria for accepting organ offers
Depending on the kind of organ needed, some factors are more important than others.
_
Each patient awaiting an organ transplant is listed on a national computerized waiting list that is maintained by the United Network for Organ Sharing (UNOS) in Richmond, Virginia. This registry contains detailed information about each patient including blood type, degree of medical urgency and other data important for matching donors to recipients. This registry changes constantly as new patients are added to the list, and as other patients either receive a transplant, die waiting, or due to a change in medical condition, are removed from the list. Specific information about each donor, including his or her blood type and body size, are entered into the national computer system. An individualized list is generated for each donor that identifies patients who match for those particular organs. There is a different list generated for each and every donor. Each available organ is allocated according to medical urgency, degree of match to the donor and time waiting. The transplant coordinator then contacts the transplant center where each potential recipient is waiting and provides detailed, confidential information about the donor. The transplant surgeon always makes the final decision about whether or not the donor and intended recipient are a good match.
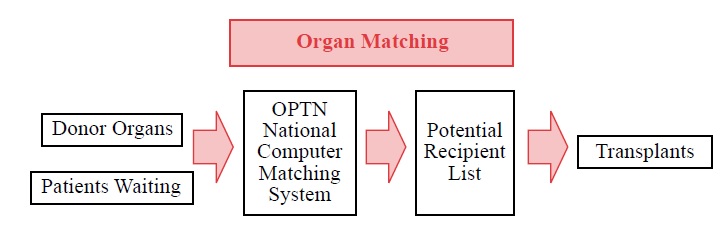
_
Average Median Wait Time to Transplant in the U.S.
- Kidney – 5 years
- Liver – 11 months
- Heart – 4 months
- Lung – 4 months
- Kidney / Pancreas – 1.5 years
- Pancreas – 2 years
In addition to deceased organ donation, patients may also receive organs from living donors. With more than 100,000 people currently waiting for a transplant in the U.S., the need for donor organs is far greater than the supply. Living donation offers an alternative for individuals awaiting transplantation.
______
Allocation of organs:
In most countries there is a shortage of suitable organs for transplantation. Countries often have formal systems in place to manage the process of determining who is an organ donor and in what order organ recipients receive available organs. The overwhelming majority of deceased-donor organs in the United States are allocated by federal contract to the Organ Procurement and Transplantation Network (OPTN), held since it was created by the Organ Transplant Act of 1984 by the United Network for Organ Sharing or UNOS. (UNOS does not handle donor cornea tissue; corneal donor tissue is usually handled by various eye banks.) Individual regional organ procurement organizations (OPOs), all members of the OPTN, are responsible for the identification of suitable donors and collection of the donated organs. UNOS then allocates organs based on the method considered most fair by the scientific leadership in the field. The allocation methodology varies somewhat by organ, and changes periodically. The overwhelming majority of deceased-donor organs in India are allocated by National Organ and Tissue Transplant Organization (NOTTO).It Functions as apex centre for All India activities of coordination and networking for procurement and distribution of Organs and Tissues and registry of Organs and Tissues Donation and Transplantation in the country.
_
Organs are allocated to transplant recipients in a fair, equitable process that takes no account of race, religion, gender, social status, disability or age – unless age is relevant to the organ matching criteria.
Criteria used in considering potential organ transplant recipients include:
- how well the organs match the person
- how long the person has been waiting for a transplant
- how urgent the transplant is
- whether the organ can be made available to the person in time.
Organs are matched to recipients by blood group, tissue compatibility, size compatibility and urgency.
_
Allocation priorities for various organs:
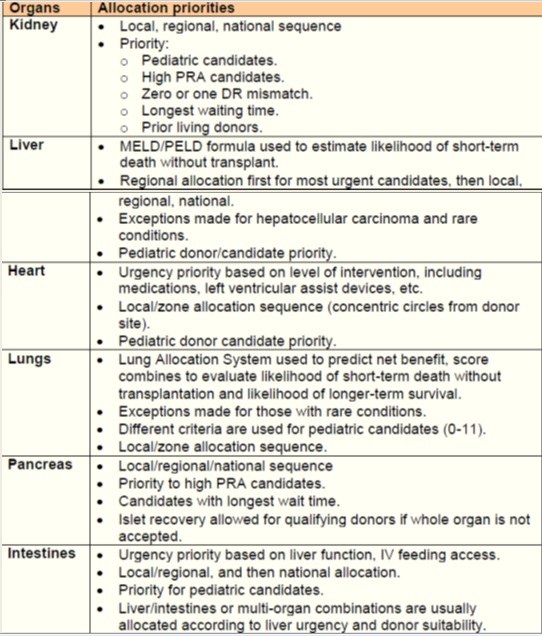
_____
_____
Organ preservation:
A deceased donor is kept on a ventilator after he or she has been declared brain dead until the organs can be harvested. A brain dead person’s organs may stay alive for a varied time period; this period may range from a couple of days to a couple of weeks. However, once the organs have been removed from the body and stored in a chemical solution, they have limited life spans. The length of time donated organs and tissues can be kept outside the body, before transplantation is to occur vary.
_
Acceptable Ischemic Times:
For the purposes of transplantation following the surgical recovery of organs, it is important to be aware of the warm and cold ischemic times. These times have an impact on the long-term survivability and function of the organ in the eventual recipient.
Warm ischemic time:
Warm ischemic time is the time a tissue, organ, or body part remains at body temperature after its blood supply has been reduced or cut off but before it is cooled. In the event of Brain Dead organ recovery, the warm ischemic time is very minimal because the time that the heart stops is virtually the same time that the organs are cooled. For a DCD organ recovery, warm ischemic time includes the amount of time that the organ is not being properly perfused prior to death, the 5 minute waiting period following death, and the time that it takes for cannulation to occur and to get the flushes and icing started. Acceptable warm ischemic times for DCD vary from transplant center to transplant center and from patient to patient.
Cold ischemic time:
Cold ischemic time refers to the time between the chilling of a tissue, organ, or body part after its blood supply has been reduced or cut off and the time it is warmed by having its blood supply restored. Cold ischemic time varies widely by organ, but in general, the sooner an organ can be transplanted, the better. Below is a list of generally accepted cold ischemic times:
- Heart: 4 hours
- Lungs: 4-6 hours
- Liver: 6-10 hours
- Pancreas: 12-18 hours
- Intestines: 6-12 hours
- Kidneys: 24 hours (may go up to 72 hours if placed on a perfusion pump following recovery)
_
In the absence of a circulation, cells rapidly switch from aerobic to anaerobic metabolism, which requires 19 times more glucose substrate to generate adenosine triphosphate (ATP) than aerobic metabolism. The result is rapid consumption of energy substrate, depletion of intracellular energy stores, and accumulation of toxic metabolites and lactic acid. As ionic membrane pumps fail for lack of ATP, the cell membrane depolarizes as sodium enters and potassium leaves the cell. Eventually, cellular integrity is lost. The purpose of organ preservation is to prevent or arrest these changes as quickly as possible. This is achieved primarily by cooling: metabolic rate is halved at temperatures below 10°C, and at 4°C is <10% of that at normal body temperature.
_
The intraoperative infusion of cold fluids is the essential first step to effective organ removal and preservation. The overriding objective with all organ transplantation is avoidance of warm ischemia. This is achieved by carefully timed and controlled in situ infusion of cold solutions into anatomical regions, the limits of which are defined by preliminary dissection of the abdominal and thoracic aorta. Organ graft cooling by the intravascular infusion of chilled solutions at the time of circulatory arrest increases the duration of organ viability and allows unhurried application, if desired, of other, more sophisticated organ preservation measures.
_
Preservation solutions for the liver, kidney, and pancreas:
Preservation solutions have been devised to counter the effects of prolonged ischaemia and minimize injury associated with reperfusion. They contain a physiological buffer to maintain pH in the face of accumulating lactic acid (e.g. phosphate or citrate) and large molecules such as mannitol or raffinose to maintain an intravascular osmotic potential in the absence of blood, thus minimizing cell swelling. In addition, the early fluids had an electrolyte composition more akin to intracellular fluid than extracellular fluid, with high potassium and low sodium concentrations to minimize diffusion. Indeed, the two most commonly used solutions today, Marshall’s solution (Soltran, a preservation solution only suitable for kidneys) and the University of Wisconsin solution (ViaSpan, suitable for the kidneys, liver, and pancreas), are high potassium, low sodium solutions. This fluid composition has implications when the organs are reperfused with blood in the recipient, since the preservation solution is washed from the transplanted organ into the circulation carrying with it its potassium load. More recent work suggests that a composition akin to intracellular fluid is not essential, and low potassium, high sodium solutions have been introduced (e.g. Celsior), although they are not widely used in the UK.
Preservation solutions for the heart and lung:
Cardiac preservation solutions tend to be adaptations of cardioplegia solutions, with a high potassium content ensuring diastolic arrest and rapid reduction of metabolic activity that is added to the effects of cooling. For pulmonary preservation, almost all centres worldwide use a low-potassium/dextran solution (commercially available as Perfadex) to which a prostaglandin vasodilator has been added, and gentle inflation of the lungs to aid perfusate distribution. Additional low-pressure retrograde perfusion via the pulmonary veins is of proven advantage, washing clot and debris out of the arterial side and possibly giving additional cooling via the bronchial circulation.
_
Cold storage:
Different organs exhibit different tolerances to warm and cold ischaemia, in part related to the nature of the organ and in part because of the demands on the organ after transplantation. Hence the heart, which has to function immediately upon transplantation, has the shortest tolerance to cold ischaemia, and each hour beyond the first results in a measurable reduction in survival; it should ideally be transplanted in <4 h. This in turn mandates that heart retrieval cannot begin until a suitable recipient has been identified, admitted to transplant centre, and indeed prepared for surgery. Although lungs are slightly more tolerant, with good function to be expected as long as cold ischaemia is <6–8 h, similar principles very often apply.
Kidneys, in contrast, need not work immediately and the recipient can be supported on dialysis until they do work. Nevertheless, there is an increased recognition that even kidneys fare better if transplanted as quickly as possible, and ideally within 18 h. The liver and pancreas lie in between and are best transplanted within 12 h. For DCD organs, those values go down to 12 and 6 h, respectively, for the kidney and liver/pancreas. Registry analysis shows that with each type of organ, the duration of cold ischaemia is one of the more significant variables in determining outcome after transplantation, and one of the only modifiable factors. Moreover, it is a continuous variable, and any period of cold or warm ischaemia is undesirable.
_
DCD and warm ischaemia:
Organ donors in whom death has been certified by neurological criteria (donation after brain death, DBD) are taken to theatre supported on a ventilator with the heart still beating. After mobilization of the organs and administration of heparin, the circulation is stopped by cross-clamping the aortic arch, draining the vena cava, and immediately flushing ice-cold preservation solution through the distal aorta thus keeping warm ischaemia, and accompanying anaerobic metabolism, to a minimum.
The organs retrieved from DCD donors are exposed to a more prolonged period of warm ischaemia than those retrieved from DBD donors. The warm ischaemic time has traditionally been assessed as the time interval between onset of irreversible asystole and subsequent cold perfusion. This time interval includes the 5 min of continuous observation required to confirm death, together with time taken to transfer the donor to the operating theatre, perform the initial laparotomy, cannulate the aorta and IVC, and begin cold perfusion. However, it is now recognized that organ hypoperfusion and warm ischaemia begin some considerable time ahead of asystole as cardiovascular and respiratory functions slowly collapse after treatment withdrawal. Thus, while the warm ischaemic time may be 10–30 min, the true ‘functional’ warm ischaemia may extend beyond an hour. With the exception of the lung (which can be inflated with oxygen immediately after entering the operating theatre), all organs that suffer warm ischaemia tolerate subsequent cold ischaemia very badly.
_
Outcomes of organs from DCD donors compared with those from DBD donors
The extra warm ischaemic damage suffered as a consequence of DCD donation manifests in different ways. For kidneys, there is an increased incidence of acute tubular necrosis that results in a delay in resumption of renal function, necessitating post-transplant dialysis in more than half of the recipients. Livers transplanted from DCD donors have a higher incidence of primary non-function requiring urgent retransplantation or resulting in death, and also more anastomotic and intrahepatic biliary strictures which may result in recurrent cholangitis and necessitate retransplantation; DCD livers are also associated with poorer graft and patient survival than DBD livers, but superior survival compared with remaining on the waiting list. There are less data for pancreas transplantation, but review of the UK Transplant Registry data suggests a higher incidence of graft thrombosis and pancreas loss with DCD donor pancreases compared with DBD donor grafts. In contrast, lungs transplanted after DCD donation function at least and also standard DBD lungs. This may be attributed to both the arrest of warm ischaemia (by prompt re-inflation of the lungs with oxygen and the resulting restoration supply of oxygen to the pulmonary alveoli) and the absence of many of the deleterious pulmonary consequences of brain-stem death such as neurogenic pulmonary oedema.
_
Improving organ preservation:
In the last two decades of organ transplantation, the focus has been on improving immunosuppression to achieve prolonged graft survival. Today, the emphasis has changed and organ preservation is being revisited in an attempt to improve outcomes. This has been spurred on by the rapid increase in DCD donation, and the use of more organs from older donors. There are several strategies that are currently being evaluated.
- Normothermic regional perfusion of the abdominal organs in DCD donation:
Surgeons in Barcelona have pioneered a technique to improve the outcomes of organs retrieved from uncontrolled DCD donors. After death, a double-balloon catheter is passed from the femoral artery into the aorta where the balloons are inflated to isolate the abdominal aorta. Venous outflow is via the ipsilateral femoral vein. The catheters are then connected to an extracorporeal membrane oxygenator (ECMO) circuit to perfuse the abdominal organs with circulating warm, oxygenated blood. This permits recovery from the warm ischaemic injury that occurs around death and early results suggest that it improves the outcomes of kidneys and livers retrieved from such donors. Having replenished ATP, the cells in the organs are then better placed to withstand subsequent cold storage. The technique has been adopted in France and in parts of the USA, and initial studies are underway in the UK in controlled DCD donors with promising early results. With the numbers of DCD donors, increasing the use of normothermic regional perfusion may become standard practice in these donors.
- Cold machine perfusion of the kidney:
After removal from the deceased donor, kidneys are usually placed in a bag of preservation solution in a box of ice, keeping the temperature of the organ around 4°C. While such static cold storage has the advantage of being simple and facilitating easy transport of the kidney from donor hospital to recipient hospital, nevertheless it has been argued that the kidney may be better preserved if it is placed on a machine where cold preservation solution is pumped through it, flushing out the small capillaries and the accumulating metabolic products. Particular attention has focused on cold machine perfusion of kidneys from DCD donors, which potentially have most to gain from improved storage.
Use of perfusion pumps:
Limitation of cold ischemic time remains the major bottleneck for the ability to use more organs or transport organs to longer distances, especially organs from marginal donors. The use of pumps to flush oxygenated fluid through the organs will help the cells to continue metabolic functions with less hypoxic injury. The use of machine perfused organs during storage allows oxygenated fluid to circulate in the tissues, allowing the cells to continue metabolism and help prevent ischemic injury. In a randomized study, cadaveric kidneys stored with machine perfusion had better outcomes than with simple cold storage. Pulsatile flow in these pumps has also been shown to improve organ function as it appears to reduce capillary pressures, increase expression of vasodilatory molecules and allow better flow of solution. In addition, other mediators like vasodilators and oxygen radical scavengers can be added to the solution on the pump. The use of pumps has dramatically improved usage and outcomes of organs, especially from marginal donors. Aside from improving function of grafts, it allows for longer cold ischemic times, and kidneys with ischemic times up to 48 hours have been utilized for transplant if they were on pump. There are currently pumps being developed for liver, heart and lung allografts as well. These pumps are portable and allow for organs to be transported while being pumped.
- Normothermic machine perfusion:
The liver: Although avoidance of unnecessary warm ischaemia is essential, there is no doubt that cold preservation is also damaging to organs, some more so than others. Steatotic (fatty) livers are particularly susceptible to damage by cold preservation, since the intrahepatic fat globules solidify and damage the hepatocytes and hepatic microcirculation, accounting in part for the high incidence of non- and poor function in such livers. One solution would be to preserve the livers at normal body temperature. Since metabolism is fully active at 37°C, such preservation needs to involve an oxygenated perfusate. Normothermic perfusion devices for the liver are currently in early trials in the UK and the first clinical transplants with such livers are expected this year. Preclinical evidence suggests that such a technique will offer considerable advantages over cold preservation, particularly for livers that have experienced significant periods of warm ischaemia as occurs in DCD donation.
The heart: The ability to extend the safe preservation period for hearts has led to much interest in normothermic perfusion. Such a device perfuses the coronary arteries and the heart itself does not need to contract; this does allow pre-transplant assessment of pump function. One such device, the TransMedics Organ Care System™ is currently undergoing phase 2 trials in the USA and has been evaluated in Europe, although the results are not yet published.
The kidney: The ability to preserve a kidney in the cold for long periods has removed the incentive to develop normothermic preservation. However, recent work suggests that a period of normothermic preservation immediately before implantation using a red cell-based plasma-free perfusate may reduce reperfusion injury; clinical trials of this are currently underway with encouraging early results.
The lung: Ex vivo lung perfusion is probably the furthest advanced of all the normothermic organ preservation techniques. Initial work showed that lungs can be perfused with a blood-based perfusate and assessed ex vivo before transplantation. The lungs are ventilated via a tracheal tube in the trachea/bronchus and perfused via a cannula in the pulmonary artery. After passing through the lungs, the perfusate passes back to an ECMO device where it is deoxygenated by a nitrogen/carbon dioxide-rich gas mixture, warmed to 37°C, and passed from there through a leucocyte filter back to the lungs. The ability of the lungs to oxygenate the perfusate gives an indication of function. There is now considerable evidence that lungs that would otherwise have been considered not suitable for transplantation could be ‘reconditioned’ ex vivo, with the potential for making significantly more lungs available for transplantation.
- Ischaemic preconditioning
Ischaemic preconditioning, either by rendering the target organ ischaemic (direct ischaemic pre-conditioning) or by rendering a different organ or tissue ischaemic (remote ischaemic preconditioning), may help reduce reperfusion injury after organ transplantation. Although animal work suggests the benefits of such an approach, there have been few large-scale trials to substantiate these observations clinically, particularly with organs from deceased donors, with the studies that have been published offering conflicting results. In part, this may reflect the very abnormal physiological state that exists after coning in brain-dead organ donors, and in part because most studies are insufficiently well powered to show any significant difference. A large correctly powered study of remote ischaemic preconditioning in living kidney donation is currently underway in the UK; large properly powered studies in deceased organ donation are awaited.
______
Super-cooling:
Researchers from Harvard University published their study in Nature about the effects of super-cooling organs. The key message of the technique is to cool organs down to -6°C degrees without allowing the development of freezing ice crystals in the preserving solutions. To preserve the organs, a special machine is used to maintain the chemical buffer zone around the organ’s cells. The buffer protects the cell’s membrane against the ice. In the experiments six rats received super-cooled livers that had been kept below 0°C for 3 days, and all of the rats survived for 3 days. If it works on human organs, it has the potential to transform organ donation. As soon as an organ is removed from the body, the individual cells it is made from begin to die. Cooling helps slow the process as it reduces the metabolic rate of the cells. Further experiments are now needed to see if the technology can be scaled up from preserving a 10g (0.35oz) rat liver to a 1.5kg (3.3lb) human liver. The researchers believe the technology could work on other organs as well.
_____
_____
How IoT helps transplant surgeons track organ shipments:
_
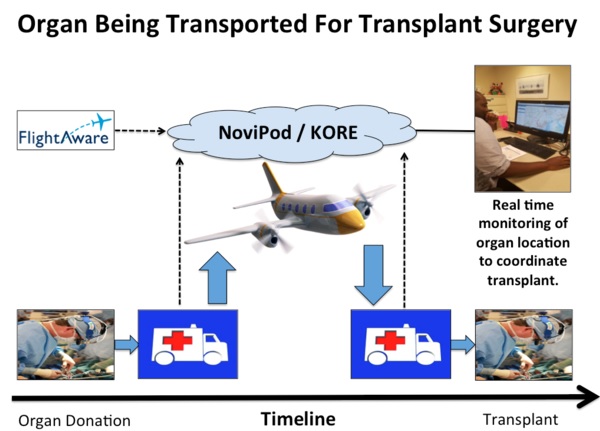
Medical teams track donated organs in real time with OrganTracker and KORE to manage the logistics of transplant surgeries:
_
There are more than 120,000 people on the United Network For Organ Sharing (UNOS) National Waiting List. Some patients have to wait up to five years for an organ donation. With so much at stake, how do you make sure a donated organ is transported safely to the recipient? The first priority goes to patients at transplant hospitals located in the same region as the donor to increase the chances of a successful transplant by doing it quickly. When there isn’t a good match locally, the organ has to be transported quickly to the transplant hospital. An ice-cold preservative solution is flushed into the organ to be donated. It is then packed in several layers of sterile containers. Each organ is accompanied by extensive paperwork documenting the details of the donor’s history and the test results from the donation surgery.
_
The OrganTracker is a web platform that uses battery-operated GPS devices to track the location and status of a donated organ while it’s being transported. A KORE SIM card that spans different cellular carriers provides connectivity. They are attached externally to the transport container to measure:
- Position in latitude and longitude coordinates
- Shocks from rapid acceleration or deceleration
- Barometric pressure: when being transported in a plane, the container is usually kept in the cockpit or managed by the flight crew
The devices send location information and the organ’s condition every five minutes to the KORE PositionLogic console. The container’s location in the air is tracked with the help of a service such as FlightAware as the devices exit cell tower range. Donated organs are viable for transplantation for four to 24 hours, depending on the type of organ. The odds of a successful transplant are improved if it is done quickly after the organ donation. The OrganTracker reduces the time needed to transport organs. A transplant coordinator closely monitors the donated organ’s location to manage the logistics, assemble the medical team and ensure that the patient is properly prepared for the transplant. UNOS reports that there are 123,000 people waiting for a transplant. IoT tracking of donated organs improve the odds of a successful transplant, but the need for donated organs is enormous. A new patient is added to the waiting list every 10 minutes. You can help by doing your part by registering as a donor today.
______
______
Immune system vis-à-vis organ donation and transplantation:
The transplantation of organs to replace diseased organs is now an important medical therapy. In most cases, adaptive immune responses to the grafted tissues are the major impediment to successful transplantation. Rejection is caused by immune responses to alloantigens on the graft, which are proteins that vary from individual to individual within a species, and are thus perceived as foreign by the recipient. In blood transfusion, which was the earliest and is still the most common tissue transplant, blood must be matched for ABO and Rh blood group antigens to avoid the rapid destruction of mismatched red blood cells by antibodies. Because there are only four major ABO types and two Rh blood types, this is relatively easy. When tissues containing nucleated cells are transplanted, however, T-cell responses to the highly polymorphic MHC molecules almost always trigger a response against the grafted organ. Matching the MHC type of donor and recipient increases the success rate of grafts, but perfect matching is possible only when donor and recipient are related and, in these cases, genetic differences at other loci still trigger rejection.
_
The primary function of the immune system is to protect the host from infectious microbes in its environment. This system has evolved over millions of years, in response of coexistence with microorganisms. Basically, the system can be divided in two components, the innate and adaptive immunities.
The innate also called natural immunity refers to a nonspecific response that involves the recruitment of diverse components of the immune system such as macrophages, neutrophils, natural killer cells (NK cells), cytokines, several cellular receptors, complement components, Toll-like receptors (TLRs), and antimicrobial peptides (AMPs). This response is phylogenetically older in comparison to the adaptive immunity, which involves recognition of specific antigen, conferring both specificity and a memory effect. The main effectors of the adaptive immunity are the T and B cells. T cells recognize antigen in the form of peptide bound to major histocompatibility complex (MHC) molecules. B cells have immunoglobulin receptors that recognize the antigenic portions of determined molecules.
In organ transplantation, the adaptive immunity is considered the main response exerted to the transplanted tissue, since the principal target of the immune response is the MHC molecules expressed on the surface of donor cells. However, we should not forget that the innate and adaptive immunities are divided only by educational purposes, since both are codependent. For example, T-cell activation leads to the production of cytokines and chemokines which in turn may recruit components of the innate immunity like NK cells or macrophages. Furthermore, local tissue production of complement components seems to be essential for full T-cell activation, and some AMPs like defensins and cathelicidin have chemoattractant properties on T lymphocytes.
_
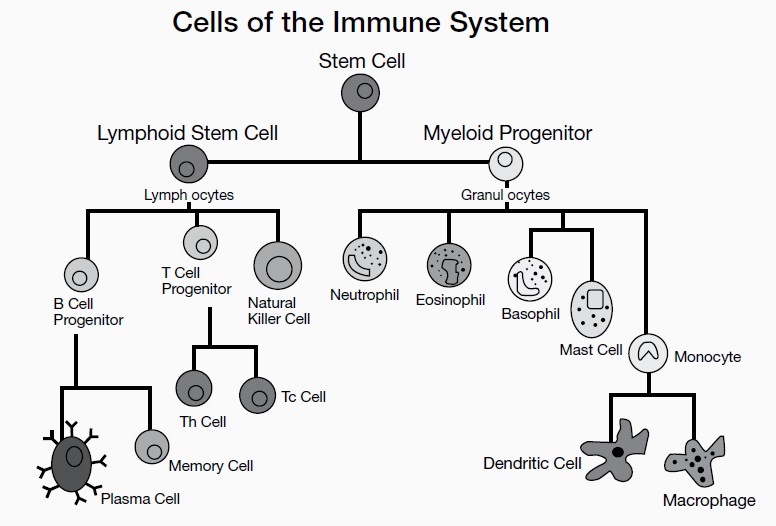
The immune system is made up of several types of white blood cells, also called leukocytes, which each have their own function.
_
Distinguishing between self and non-self:
Because the immune system uses many different effector mechanisms to destroy the broad range of microbial cells and particles that it encounters, it is critical for the immune response to avoid unleashing these destructive mechanisms against its own tissues. This avoidance of destruction of self-tissues is referred to as self-tolerance. Mechanisms to avoid reaction against self-antigens are expressed in many parts of both the innate and the adaptive immune responses. Failure of self-tolerance underlies the broad class of autoimmune diseases. Unfortunately, transplanted tissues from individuals of the same species (allogenic) or different species (xenogeneic) are recognized as non-self, causing graft rejection. The process by which the immune system recognizes pathogens, tumors, and transplantation antigens involves the same antigen recognition molecules.
Major histocompatibility complex (MHC) is clusters of genes on the short arm of chromosome 6 expressed on the cell surface as HLA antigens i.e. genes that encode HLA. HLA antigens- are most common cause of graft rejection. HLA A, B (Class I) and DR (class II) are most important in organ transplant. Anti HLA antibodies may cause hyperacute rejection. CD8+ and CD4+ recognize HLA class 1 and 2 antigens respectively.
_
When the immune system encounters a foreign organism, it mounts an attack against it to protect the body from infection. To prevent an attack on our own cells and tissues (autoimmunity), the immune system must be able to differentiate between our own healthy tissues and foreign invaders. Foreign invaders are presented to the immune system in the form of small molecules called antigens. Identification of these non-self antigens will trigger an immune response and will stimulate the production of antigen specific antibodies that mark infected cells for destruction by the immune system and help amplify the immune response. The Human Leukocyte Antigen (HLA) complex is a group of genes that encode the proteins responsible for identifying foreign agents to the immune system. These proteins are found on the surface of all cells and act as ‘self-markers’ telling the immune system not to trigger a response. Each person will have their own specific set of HLA proteins, based upon their unique genetic make-up, that the immune system will have learned not to react to. Any cell not displaying these specific HLA proteins will be identified as ‘non-self’ by the immune system and will be treated as a foreign invader.
_
Self-antigens are products of a group of linked genes, known as the Major Histocompatibility complex (MHC). They are found on almost every nucleated cell in your body, however they are particularly seen on antigen-presenting cells. MHC molecules are small glycoproteins that are presented on a cell surface. They are the only molecule capable of presenting an antigen to a T cell. MHC molecules are the antigens which play a main role in transplant rejection. Since MHC molecules are specific to the individual, when we transplant organs, the immune system sees this antigen and recognises it as non-self.
_
Only identical twins have the same MHC markers, making the success rate of transplants between them, extremely high. In all other combinations, the tissue between recipient and donor must be analysed. Often members of the same family will have similar antigen markers, making the chances for success slightly higher. Red blood cells however have significantly less MHC molecules (non-nucleated). This is why blood transfusions are more successful than organ transplants. However even when success rates are high and an excellent match has been found, it is still important to use immunosuppressive drugs. These drugs suppress and reduce the strength of the immune system. However while on these the individual is a high risk for infections and developing cancers.
_
Transplantation Antigens:
The rejection response to grafted tissue is caused by cell surface molecules that induce an antigenic stimulus. A wide variety of transplantation antigens have been described, including the MHC molecules, minor histocompatibility antigens, ABO blood group antigens, and monocytes/endothelial cell antigens. The minor histocompatibility antigens are processed peptides derived from cellular antigens that are presented by MHC molecules but are not derived from the MHC. The response to minor H antigens is in most ways analogous to the response to viral infection. However, an antiviral response eliminates only infected cells, whereas all cells in the graft express minor H antigens, and thus the entire graft is destroyed in the response against these antigens. Thus, even though MHC genotype might be matched exactly, polymorphism in any other protein could elicit potent T-cell responses that would destroy the entire graft. It is no wonder that successful transplantation requires the use of powerful immunosuppressive drugs. ABO compatibility is of much less importance than MHC compatibility in graft survival. However, ABO incompatibility can result in hyperacute rejection of primarily vascularized grafts, such as kidney and heart. As we mentioned before, the principal target of the transplantation immune response is the MHC molecules expressed on the surface of donor cells.
Alloantigen is an antigen that differs between members of the same vertebrate species, such as HLA molecules and blood group antigens. Alloantigens are determined by the different alleles of polymorphic genes. Immunogenetics is a subfield of immunology that deals with the polymorphism and population genetics of genes and proteins that are important for immune system function.
_
Graft rejection occurs when the recipient’s immune system attacks the donated graft and begins destroying the transplanted tissue or organ. The immune response is usually triggered by the presence of the donor’s own unique set of HLA proteins, which the recipient’s immune system will identify as foreign. The degree of similarity between the HLA genes of the donor and recipient is known as histocompatibility; the more genetically compatible the donor and the recipient, the more tolerant the recipient’s immune system should be of the graft. However, unless the donor and recipient are genetically identical (e.g. as in identical twins) there will always be some degree of rejection. As well as non-self HLA proteins, other surface proteins on the donor graft can also be identified as a foreign antigen and illicit an immune response. In some cases, a patient may experience something known as ‘graft versus host reaction’ where mature immune cells already present in the donor graft begin attacking the healthy cells of the recipient. Graft versus host reaction, where the donor graft is described as being “immune-competent” (i.e. capable of producing an immune response) is a particular risk with stem cell transplants (bone marrow transplant) and can also occur following blood transfusions.
_
MHC/HLA system:
The most important genes deciding the fate of a transplanted cell, tissue, or organ belong to what is termed the MHC (the major histocompatibility complex). The MHC was first identified through tumor transplantation studies in mice by Peter Gorer in 1937. In 1980 George Snell, Jean Dausset and Baruj Benacerraf received the Nobel Prize in Physiology or Medicine for their contributions to the discovery and understanding of the MHC. World Health Organization Nomenclature Committee designated that the leukocyte antigens controlled by the closely linked genes of the human MHC be named HLA (for human leukocyte antigen). The MHC is the most highly polymorphic genetic system expressed in people. By “polymorphic” is meant that there are multiple forms of the gene (polymorphisms) occurring at a given gene locus. The chance for unrelated people to be MHC-identical is low. The main function of the MHC antigens is peptide presentation to the immune system to help distinguish self from non-self. These antigens are called HLA (human leukocyte antigens).
_
The need for HLA matching depends on the type of transplant. In bone marrow transplantation, HLA matching is an absolute necessity, lest the cells be rejected. In corneal transplantation, HLA matching is less relevant because of the lack of blood vessels in the cornea and the “immunological privilege” of the cornea. HLA matching is not crucial but is beneficial to the success of most solid organ transplantation including kidney, liver, heart, lung, pancreas, and intestine.
_
With the three highly polymorphic MHC I genes in humans (HLA-A, HLA-B, and HLA-C) determining compatibility, each with many alleles segregating in a population, odds are extremely low that a randomly chosen donor will match a recipient’s six-allele genotype (the two alleles at each locus are expressed codominantly). This is why a parent or a sibling may be the best donor in many situations—a genetic match between the MHC genes is much more likely and the organ is much less likely to be rejected. Although matching all of the MHC genes can lower the risk for rejection, there are a number of additional gene products that also play a role in stimulating responses against grafted tissue. Because of this, no non-self grafted tissue is likely to completely avoid rejection. However, the more similar the MHC gene match, the more likely the graft is to be tolerated for a longer time. Most transplant recipients, even those with tissues well matched to their MHC genes, require treatment with immunosuppressant drugs for the rest of their lives. This can make them more vulnerable than the general population to complications from infectious diseases. It can also result in transplant-related malignancies because the body’s normal defenses against cancer cells are being suppressed.
_
The major antigens in mammalian species are encoded by a closely linked series of genes called MHC. In humans, these genes reside in the short arm of chromosome 6. The MHC complex contains a number of genes that control several antigens, most of which influence allograft rejection. These antigens (and their genes) can be divided into three major classes: class I, class II and class III. The class I and class II antigens are expressed on cells and tissues whereas as class III antigens are represented on proteins in serum and other body fluids (e.g.C4, C2, factor B, TNF). Antigens of class III gene products have no role in graft rejection.
_
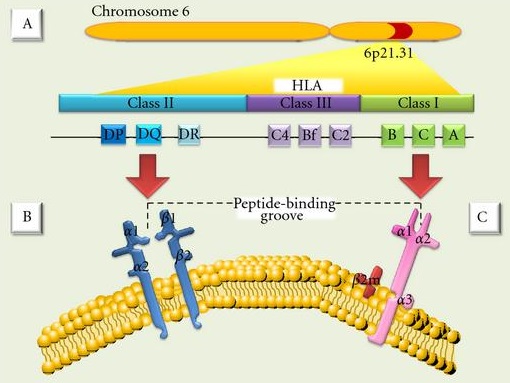
Figure above shows (A) MHC (major histocompatibility complex). (B) Class II antigens are expressed only on B lymphocytes, activated T lymphocytes, monocytes, macrophages, Langerhans cells, dendritic cells, endothelium, and epithelial cells. They are heterodimers composed of noncovalently associated α and β polypeptide chains encoded by genes of the HLA-D region. (C) Class I MHC antigens are present on all nucleated cells and are composed of a 45-kd transmembrane α heavy chain encoded by genes of the HLA-A, HLA-B, or HLA-C loci on chromosome 6.
_
In transplantation immunology, the major impact in graft loss comes from the effects of HLA-A, B and -DR antigens. There also appears to be a temporal HLA mismatching effect. HLA-DR mismatch effect is the most important in the first 6 months after transplantation, the HLA-B effect emerges in the first 2 years, and HLA-A mismatches have a deleterious effect on long-term graft survival.
_
Inheritance:
HLA antigens are inherited in a Mendelian co-dominant manner. HLA genes are almost always inherited together, thus the antigens of the entire HLA region inherited from one parent collectively are called haplotype. MHC genes are inherited as a group (haplotype), one from each parent. Thus, a heterozygous human inherits one paternal and one maternal haplotype, each containing three class-I (B, C and A) and three class II (DP, DQ and DR) loci.
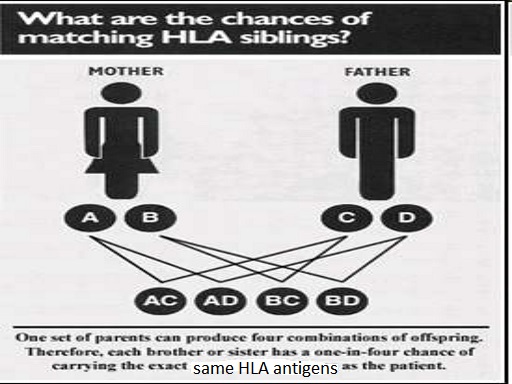
Because chromosome 6 is an autosome (a chromosome with two pairs), all individuals have two HLA haplotypes (one for each chromosome). According to this, any sibling pair has a 25% chance of inheriting the same two parental haplotypes, a 50% chance of sharing one haplotype, and a 25% chance of having two completely different haplotypes. All children are haploidentical with each parent.
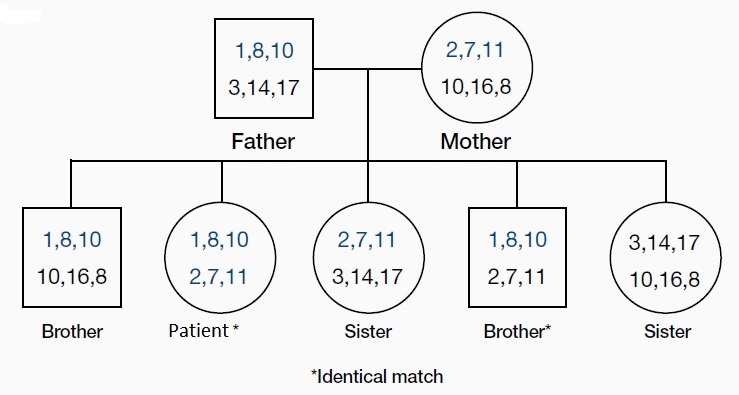
Organs transplanted between MHC identical individuals are readily accepted, whereas organs transplanted between MHC antigen-mismatched individuals are rejected in the absence of immunosuppressive therapy.
_
Crossover:
Haplotypes, normally, are inherited intact and hence antigens encoded by different loci are inherited together (e.g., A2; B27; Cw2; DPw6; DQw9; DRw2). However, on occasions, there is crossing over between two parental chromosomes, thereby resulting in new recombinant haplotypes. Thus, any one specificity encoded by one locus may combine with specificities from other loci. This results in vast heterogeneity in the MHC make-up in a given population.
______
Two distinct types of alloreaction can occur in clinical transplantation:
- Transplant rejection
- Graft- versus- host disease (GVHD)
_
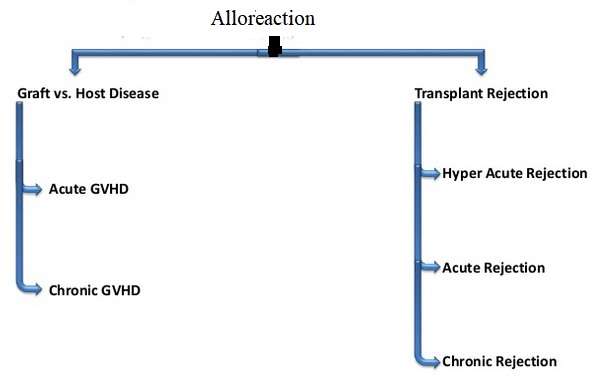
_
Transplant rejection is an immune reaction that is directed toward transplanted tissue from a genetically non-identical donor and leads to death of the graft. Graft versus host reaction is the response of mature donor-derived T cells in transplanted bone marrow or other type of hematopoietic cell transplant to the alloantigens of the recipient’s tissues. White blood cells of the donor’s immune system which remain within the donated tissue (the graft) recognize the recipient (the host) as foreign (non-self). The white blood cells present within the transplanted tissue then attack the recipient’s body’s cells, which leads to GVHD. This should not be confused with a transplant rejection, which occurs when the immune system of the transplant recipient rejects the transplanted tissue; GVHD occurs when the donor’s immune system’s white blood cells reject the recipient. The underlying principle (alloimmunity) is the same, but the details and course may differ. Transfusion-associated graft-versus-host disease (TA-GVHD) is a rare complication of blood transfusion, in which the donor T lymphocytes mount an immune response against the recipient’s lymphoid tissue. Donor lymphocytes are usually identified as foreign and destroyed by the recipient’s immune system. However, in situations where the recipient is immunocompromised, or when the donor is homozygous and the recipient is heterozygous for an HLA haplotype (as can occur in directed donations from first-degree relatives), the recipient’s immune system is not able to destroy the donor lymphocytes. This can result in graft-versus-host disease.
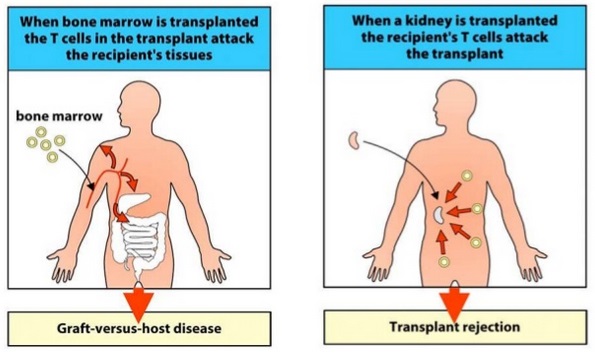
_____
The Allogeneic Immune Response:
The phenomenon by which the recipient immune system reacts with donor antigens that are considered to be “non-self” is named allorecognition. The main and strongest responses to alloantigens are mediated by host T cells, which recognize peptide antigens presented in the context of MHC, by antigen-presenting cells (APCs). However, evidence that the innate alloimmunity has an important role in graft rejection has recently been proposed by Land and coworkers. They state in their “Injury Hypothesis” that initial allograft injury reflected by reactive oxygen species (ROS) during reperfusion is associated with generation of DAMPs (meaning damage-associated molecular patterns) such as heat shock proteins (HSP) and hyaluronan fragments (fHA) among others, all of which are recognized by TLR4 and/or TLR2. Subsequent TLR4 and TLR2-triggered signalling pathways utilize adaptor proteins including MyD88 (myeloid differentiation marker 88), which in turn initiate downstream signalling pathways that lead to activating the 3 master transcription factors NF-κB (nuclear factor-kappa B), AP-1 (activator protein-1), and IRF-3 (interferon regulatory factor 3). NF-κB seems mainly to be responsible for maturation of donor-derived and recipient-derived dendritic cells, which represents the bridge to development of an adaptive alloimmune response that results in rejection.
_
Co-stimulation of T and B lymphocytes:
During the activation of lymphocytes, co-stimulation is often crucial to the development of an effective immune response. Co-stimulation is required in addition to the antigen-specific signal from their antigen receptors. T cells require two signals to become fully activated. A first signal, which is antigen-specific, is provided through the T cell receptor (TCR) which interacts with peptide-MHC molecules on the membrane of antigen presenting cells (APC). A second signal, the co-stimulatory signal, is antigen nonspecific and is provided by the interaction between co-stimulatory molecules expressed on the membrane of APC and the T cell. Th2 cell can co-stimulate the B cell. Without this co-stimulation the B cell cannot proliferate further. Co-stimulation for B cells is provided alternatively by complement receptors.
_
Are dendritic cells antigen presenting cells?
Yes. The expression of co-stimulatory molecules and MHC class II are defining features of professional APCs. All professional APCs also express MHC class I molecules as well. The main types of professional antigen-presenting cells are dendritic cells, macrophages and B cells. Non-professional antigen presenting cells include all nucleated cell types in the body.
_
Direct and indirect allorecognition:
Unique to transplant immunobiology is the idea that alloantigen recognition can occur via two distinct pathways, both of which focus on the source of the antigen presenting cells (donor versus recipient). The direct pathway of allorecognition describes the ability of T cells to “directly” recognize intact non-self MHC molecules present on the surface of donor cells. The indirect pathway of allorecognition describes the ability of T cells to recognize donor MHC molecules that are processed and presented as peptides by self-MHC molecules. The recognition of intact donor MHC molecule(s) elicits a potent anti-graft immune response while processed MHC peptides and minor histocompatibility antigens elicit a slower tempo, less intense immune response.
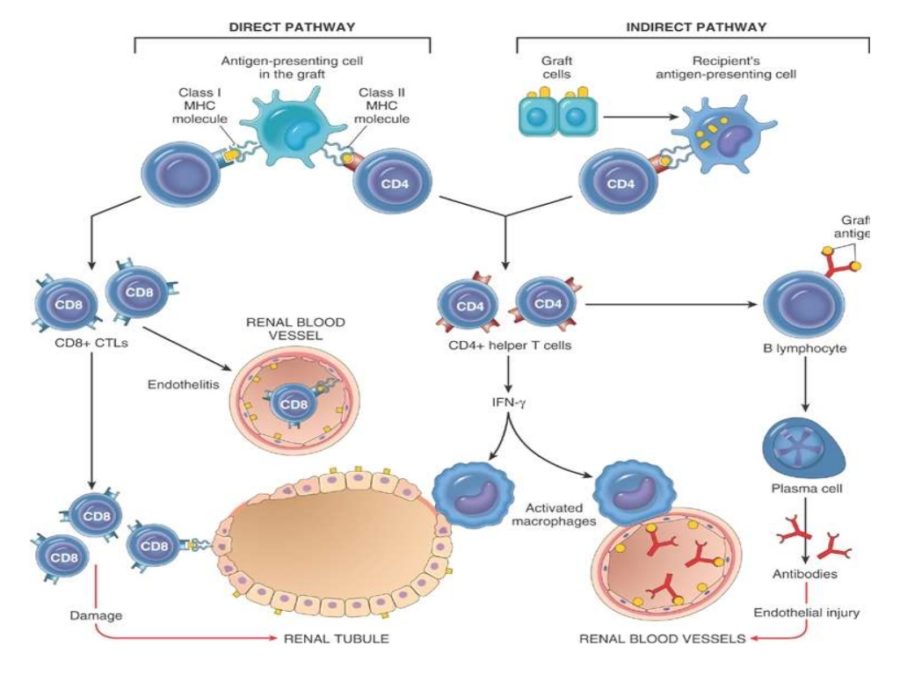
Figure above shows two distinct pathways of allorecognition.
Left- Direct pathway of allorecognition. Dendritic cells (donor APCs) migrate from the graft to secondary lymphoid tissues to activate T cells.
Right- Indirect pathway of allorecognition. Graft proteins are processed by recipient dendritic cells and presented to T cells.
_
Organ grafts carry with them antigen-presenting cells of donor origin, known as passenger leukocytes, and these are an important stimulus to alloreactivity. This route for sensitization of the recipient to a graft seems to involve donor antigen-presenting cells leaving the graft and migrating via the lymph to regional lymph nodes. Here they can activate those host T cells that bear the corresponding T-cell receptors. The activated alloreactive effector T cells are then carried back to the graft, which they attack directly. Indeed, if the grafted tissue is depleted of antigen-presenting cells by treatment with antibodies or by prolonged incubation, rejection occurs only after a much longer time. Also, if the site of grafting lacks lymphatic drainage, no response to the graft results.
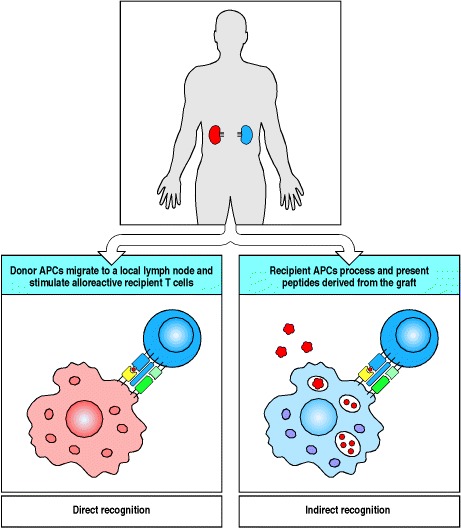
A second mechanism of allograft recognition leading to graft rejection is the uptake of allogeneic proteins by the recipient’s own antigen-presenting cells and their presentation to T cells by self MHC molecules. The recognition of allogeneic proteins presented in this way is known as indirect allorecognition, in contrast to the direct recognition by T cells of allogeneic MHC class I and class II molecules expressed on the graft itself. Among the graft-derived peptides presented by the recipient’s antigen-presenting cells are the minor H antigens and also peptides from the foreign MHC molecules themselves, which are a major source of the polymorphic peptides recognized by the recipient’s T cells.
_
Allorecognition is initiated by CD4+ and CD8+ T cells recognizing either intact allo-MHC molecules (MHC class II and I, respectively) on donor antigen-presenting cells (APCs) (direct pathway) or allopeptides bound to self-MHC molecules on recipient APCs (indirect pathway) where presentation may occur via MHC class I or MHC class II, although class II is usually involved. The cells that respond to minor H antigens are generally CD8+ T cells, implying that most minor H antigens are complexes of donor peptides and MHC class I molecules. However, peptides bound to MHC class II molecules can also participate in the response to MHC-identical grafts. The relative contributions of direct and indirect allorecognition in graft rejection are not known. Direct allorecognition is thought to be largely responsible for acute rejection, especially when MHC mismatches mean that the frequency of directly alloreactive recipient T cells is high. Furthermore, a direct cytotoxic T-cell attack on graft cells can be carried out only by T cells that recognize the graft MHC molecules directly. Nonetheless, T cells with indirect allospecificity can contribute to graft rejection by activating macrophages, which cause tissue injury and fibrosis, and are likely to be important in the development of an alloantibody response to a graft.
_
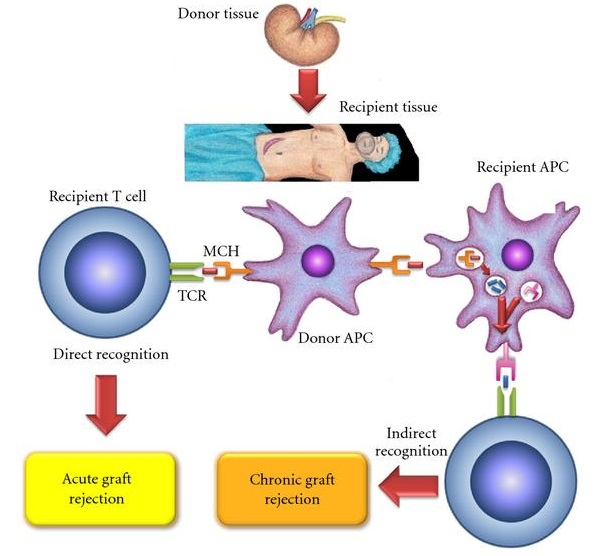
Figure above shows Allogeneic immune response: this could happen by three recognizing mechanisms: first, an indirect recognition: this type of mechanism has a dominant role in chronic rejection; second, a direct recognition: this mechanism determines a strong immune response in the acute rejection; third mechanism, a “semi-direct” recognition that could be mediated by immunoglobulin-like receptors of natural killer (NK) cells and can mediate potent acute rejection.
_
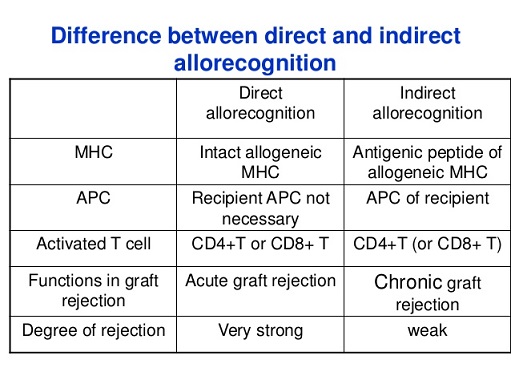
_
Recently, it was shown that both naïve and memory CD4+ and CD8+ T cells are frequently cross-reactive against allogeneic HLA molecules and that this allorecognition exhibits exquisite peptide and HLA specificity. Such advances in the understanding of the immunogenetics of allorecognition have led some researches to suggest a new model for allorecognition whereby the majority of T cell alloresponses may occur via direct recognition (cross-reactivity) by thymically educated naïve and memory T cells against allogeneic HLA molecules presenting self-peptides. According to this model, thymically educated T cells are commonly and specifically allo-HLA reactive and are activated by viral infection or vaccination to become alloreactive memory T cells which are a major barrier to successful tolerance.
_
Transplant rejection:
Transplant rejection or allograft rejection is a normal process in which the functional immune system of a transplant recipient attacks the transplanted organ or tissue. ‘Rejection’ means that someone’s body recognises that the transplanted kidney is not ‘its own’ and tries to ‘reject’ it from the body. Even when someone is ‘well matched’ with their transplant kidney (in terms of blood group and tissue type), some degree of rejection (approximate risk is 15 out of 100 transplants) is common. The severity of rejection varies from patient to patient. There are three general forms of rejection: hyperacute, acute, and chronic. “Hyperacute” rejection occurs within minutes of transplantation due to antibodies in the organ recipients blood stream that react with the new organ and result in organ failure within the first hours after transplantation. The kidney and heart are most susceptible to this problem, the liver is relatively resistant. Hyperacute rejection has not been sufficiently studied in pancreas or lung transplantation. Cross matches are done between a particular kidney and a potential recipient of that kidney to decrease the likelihood that hyperacute rejection will occur. “Acute” rejection generally occurs in the first 6 to 12 months after transplantation. Lymphocytes from the thymus (t-cells) are blamed for causing acute rejection. For most organs, the only way to show unequivocally that rejection is occurring is by biopsy of that organ. For practical reason, however, biopsies are not always done when acute rejection is suspected. In some circumstances treatment for rejection is begun and a biopsy is performed at a later date if the organ doesn’t seem to be improving. This strategy varies from organ to organ and transplant center to transplant center. The diagnosis and treatment of acute rejection can be extremely difficult at times. Chronic rejection is less well defined than either hyperacute or acute rejection. It is probably caused by multiple factors: antibodies as well as lymphocytes. The definitive diagnosis of chronic rejection is again generally made by biopsy of the organ in question. The heart is an exception to this generalization: chronic rejection in heart grafts is felt to be manifest by accelerated graft atherosclerosis. In other words, the transplanted heart rapidly develops “hardening of the arteries”. Kidneys with chronic rejection have fibrosis (scarring) and damage to the microscopic blood vessels in the substance of the kidney. Livers with chronic rejection have a decreased number of bile ducts on biopsy. This is referred to as the “vanishing bile duct syndrome”. Transplanted lungs with chronic rejection are said to have “bronchiolitis obilterans” a scarring problem in the substance of the lung.
_
Rejection is the major barrier to successful transplantation. The immune response to an allograft is an ongoing dialogue between the innate and adaptive immune system that if left unchecked will lead to the rejection of transplanted cells, tissues, or organs. Activation of elements of the innate immune system, triggered as a consequence of tissue injury sustained during cell isolation or organ retrieval and ischemia reperfusion, will initiate and amplify the adaptive response. T cells require a minimum of two signals for activation, antigen recognition, and costimulation. The activation requirements of naive T cells are more stringent than those of memory T cells. Memory T cells are present in the majority of transplant recipients as a result of heterologous immunity. The majority of B cells require help from T cells to initiate antibody production. Antibodies reactive to donor human leukocyte antigen molecules, minor histocompatibility antigens, endothelial cells, RBCs, or autoantigens can trigger or contribute to rejection early and late after transplantation. Antibody-mediated rejection triggered by alloantibody binding and complement activation is recognized increasingly as a significant contribution to graft loss. Acute and chronic antibody-mediated rejections (AMR) are playing an increasingly critical role in kidney allograft loss and are considered among the most important barriers that limit long-term outcomes. Even though one component of the immune system may dominate and lead to rejection being described in short hand as T cell or antibody mediated, it is usually multifactorial resulting from the integration of multiple mechanisms. Identifying the molecular pathways that trigger tissue injury, signal transduction and rejection facilitates the identification of targets for the development of immunosuppressive drugs.
_
Leukocytes and cytokines in graft rejection:
Allograft rejection results from the coordinated activation of alloreactive T cells and antigen-presenting cells (APCs). Although acute rejection is a T-cell–dependent process, the destruction of the allograft results from a broad array of effector immune mechanisms. Cell-cell interactions and the release by primed helper T cells of multiple types of cytokines (interleukin [IL]-2, IL-4, IL-5, IL-7, IL-10, IL-15, tumor necrosis factor-α, and interferon-γ) recruit not only immunocompetent donor-specific CD4+ T cells, CD8+ cytotoxic T cells, and antibody-forming B cells but also nonspecific inflammatory cells, which constitute the majority of cells infiltrating an allograft. Other cells specific to the transplanted organ may play a role in the balance of tolerance and rejections, such as the Kupffer cells and the sinusoidal epithelial cells in the liver. Stimulation of CD4+ T cells through their antigen receptors is not sufficient to initiate T-cell activation, unless costimulation is provided by interaction of other ligand-receptor pairs present on the surfaces of T cells and APCs during the encounter. Some of these interactive pairs include the T-cell surface molecule CD2 and its ligand CD58 on APCs; CD11a/CD18:CD54; CD5:CD72; CD40L:CD40; and CD28:CD80 or CD86. CD4+ T-cell anergy or tolerance induction occurs when the T-cell receptor interacts with the APC unless signals are provided through one or more of these receptor-ligand interactions (particularly through CD40L:CD40 and CD28:CD80 or CD86) or by cytokines (such as IL-1 and IL-6 from the APC). Thus, T-cell accessory proteins and their ligands on APCs are target molecules for antirejection therapy. If costimulation does occur, the CD4+ T cell becomes activated, which leads to stable transcription of genes important in T-cell activation. CD8+ T cells recognize antigenic peptides displayed on MHC class I molecules and represent a major cytotoxic effector lymphocyte population in graft rejection. Donor class I molecules on donor APCs in the graft directly activate cytotoxic effector lymphocytes. However, CD8 activation also requires a costimulatory second signal, as well as an IL-2 signal. Activated CD8+ T cells proliferate and mature into specific alloreactive clones capable of releasing granzyme (serine esterase), perforin, and toxic cytokines, such as tumor necrosis factor-α. More recently, the identification of TH17 effector cells (pro-inflammatory) and regulatory T cells (down-regulate immune activation) has improved our understanding of the development of graft tolerance or rejection. Stimulation of the B cell by antigen occurs through its antigen receptor (surface immunoglobulin), but costimulation is also required for B-cell activation. This costimulation can be provided by cytokines released by T cells or through many of the same T-cell protein-ligand pairs important in T-cell–APC costimulation, because these ligands are also present on B cells. B cell contribution to the immune rejection of organ transplants is not limited to the production of alloimmune antibodies, but also involves antigen presentation and the secretion of proinflammatory cytokines. Once T-cell activation has occurred, autocrine T-cell proliferation continues as a consequence of the expression of the IL-2 receptor (IL-2R). Interaction of IL-2 with its receptor triggers the activation of protein tyrosine kinases and phosphatidylinositol-3-kinase, resulting in translocation into the cytosol of an IL-2R–bound serine-threonine kinase, Raf-1. This in turn leads to the expression of several DNA-binding proteins, such as c- Jun, c-Fos, and c-Myc, and to progression of the cell cycle. The consequence of all of these events is the development of graft-specific, infiltrating cytotoxic T cells. Cytokines from the T cells also activate macrophages and other inflammatory leukocytes and cause upregulation of HLA molecules on graft cells. The activated T cells also stimulate B cells to produce antigraft antibodies. Ultimately, if not recognized and managed, all these cellular and humoral factors constitute the rejection process that destroys the graft.
_______
Role of the Transplant in initiating Rejection through activation of recipient innate immunity:
Traditionally, the recognition and tolerance of transplanted grafts has been considered to be within the realm of the adaptive immune system. Innate immunity, on the other hand, as the first line of host defense, plays a role in fighting against invading microorganisms. Recently, with the discovery of the Toll‐like receptors (TLRs), the role of innate immune responses in the control of adaptive immunity has become a new area of interest. Emerging evidence suggests that in addition to responding to pathogen‐associated molecular patterns of microorganisms, TLRs can be activated by endogenous ligands, expressed by mammalian cells. These ‘danger signals’ may participate in ischemia‐reperfusion related organ damage and subsequently influence function and survival of transplanted grafts. Furthermore, it has been suggested that adaptive immune responses can enhance the acute inflammatory responses controlled by innate immunity in organ transplantation.
_
Innate Immune Activation in Transplantation-Tissue Injury:
Tissue injury during the pre- and posttransplant periods may result from a multitude of mechanisms, and these factors contribute to end-organ damage and affect allograft survival. Immune activation in the donor organ during the pretransplant period begins with brain death and the neuropathology associated with brainstem herniation. As the medulla becomes ischemic, vagal activity ceases, resulting in massive sympathetic outflow and high levels of catecholamines. In addition to affecting cardiac function by stimulating tachycardia, hypertension, and dysrhythmia, catecholamine release results in peripheral vasoconstriction that can contribute to end-organ ischemia. Following the resolution of the catecholamine storm, the sympathetic tone is lost, resulting in vasodilatation and reperfusion injury to tissue followed by hypotension that can again cause organ hypoperfusion. Brain death also results in an outpouring of inflammatory cytokines, including IL-6 that has been shown to correlate with worse recipient outcomes in the setting of kidney transplantation.
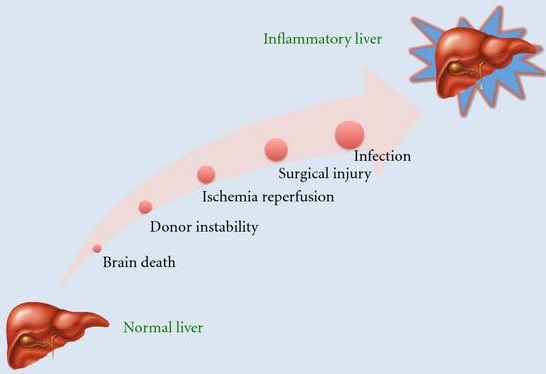
Figure above shows that Liver injury during transplantation can convert an immunologically quiescent organ to an inflammatory organ that promotes acute rejection. The physical process of isolating and manipulating cells or removing, reimplanting, and reperfusing tissue or organs for transplantation initiates injury and stress responses, resulting in changes in gene and protein expression and folding within the donor tissue that have a profound influence on the immunological response of the recipient. In the case of deceased organ donors some of these changes are also a direct consequence of brain or cardiac death. Although organ preservation, perfusion, or preconditioning strategies can ameliorate some of these events, they cannot, as yet, prevent all tissue damage and activation of the innate immune system.
_
Innate immune responses are the consequence of several events associated with clinical transplantation, such as ischemia-reperfusion injury and infections, and lead to the release of damage-associated molecular patterns (DAMPs) and pathogen-associated molecular patterns (PAMPs) (Chong and Alegre 2012). Local tissue damage and ischemia reperfusion injury generates many potential DAMPS, including reactive oxygen species, heat shock proteins, heparin sulfate, high mobility group box-1 after capture by the receptor for advanced glycation end products complex and fibrinogen, that can bind to PRRs. DAMPs and PAMPs are recognized by so-called pattern-recognition receptors (PRRs) expressed by hematopoietic cells. The specificity of PRRs is genetically determined and several subgroups can be classified based on their structure. The transmembrane group of PRRs includes several families of molecules such as toll-like receptors (TLRs), C-type lectins, RAGE (receptor for advanced glycation endproducts), complement receptors, scavenger receptors, and mannose receptors. The cytosolic PRR group includes retinoic acid-inducible gene-I-like receptors and nucleotide-binding domain and leucine-rich repeat-containing receptors (Iwasaki and Medzhitov 2010).
_
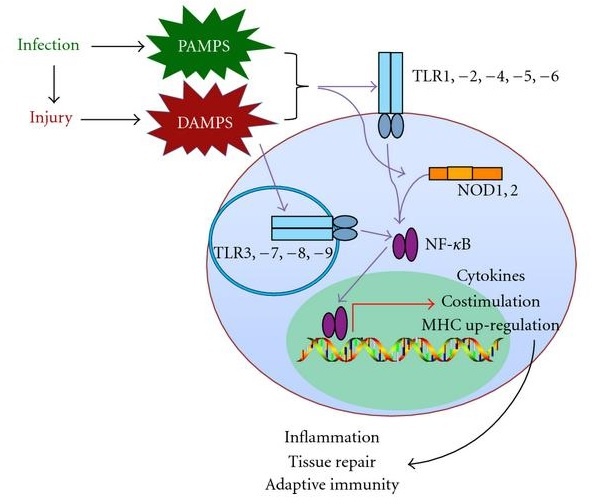
Figure above shows infection and cell injury result in the production of PAMPs and DAMPs that promote the inflammatory response via TLRs located on the cell membrane and within endosomes. Cytoplasmic PAMPs activate similar pathways by binding to NOD1 and NOD2.
Immediately after transplantation, PRR-mediated danger signals activate dendritic cells (DCs) (LaRosa et al. 2007) leading to antigen-presenting cell (APC) maturation, up-regulation of costimulatory molecules, and secretion of proinflammatory cytokines. In this context, donor APCs migrate to the T cell areas of secondary lymphoid organs and induce the activation and differentiation of alloreactive naïve T cells into effector T helper cells. These effector cells migrate into the graft where they activate macrophages and granulocytes (neutrophils, eosinophils, and basophils) that have infiltrated the graft in response to inflammatory stimuli. The latter cells contribute to lesion formation, either directly or through the production of proinflammatory cytokines and chemokines. They also help boost and maintain the adaptive immune T-cell response. The end result is the production of inflammatory mediators including the proinflammatory cytokines, interleukin (IL)-1, IL-6, and tumor necrosis factor (TNF), type I interferons, chemokines (chemoattractant cytokines), and the rapid expression of P-selectin (CD62P) by endothelial cells. These events identify the transplant as a site of injury and inflammation modifying the activation status, permeability, and viability of endothelial cells lining the vessels, triggering the release of soluble molecules, including antigens from the graft, inducing the production of acute phase proteins including complement factors systemically and in some cases by the organ itself, stimulating the migration of donor-derived antigen presenting cells (APCs) including dendritic cells, from the transplant to recipient lymphoid tissue, and triggering the recruitment of inflammatory leukocytes into the graft. Another cell type involved in innate immunity is the NK cell. In a proinflammatory context, NK cells become activated and are able to kill target cells (Pratschke et al. 2009). The complement system plays a central role in the effector mechanisms occurring during the innate response. The three complement pathways (classical, alternative, and mannose lectin) can be activated by DAMPs as well as by the inflammatory environment that develops during ischemia reperfusion injury (Castellano et al. 2010). Moreover, the intermediate product of complement, C5a, is able to bind to APC receptors, leading to Th1 activation and development of the adaptive immunity (Zhou et al. 2000).
__
Activation of the innate immune system in the early phase posttransplant is largely, a non-specific response to tissue damage and will occur, irrespective of whether there is a genetic difference between the donor and recipient. An emerging body of evidence suggests that innate immunity, providing the first line of host defence against invading pathogens or their components (PAMPs), also plays a critical role in acute and chronic allograft rejection. Donor organ injury induces an inflammatory milieu in the allograft, and this appears to be the initial key event for activation of the innate immune system. Injury-induced generation of putative endogenous molecular ligand, in terms of damage/danger-associated molecular patterns (DAMPs) such as heat shock proteins, are recognized by toll-like receptors (TLRs). Acute allograft injury such as oxidative stress during donor brain-death condition and post-ischemic reperfusion injury in the recipient could induce DAMPs, which may activate innate TLR-bearing dendritic cells (DC), which could initiate the recipient´s adaptive alloimmune response leading to acute allograft rejection. Chronic injurious events in the allograft induce the generation of DAMPs, which may interact with and activate innate TLR-bearing vascular cells (endothelial cells, smooth muscle cells), contributing to the development of atherosclerosis of donor organ vessels and promoting chronic allograft rejection. In this manner, the transplant itself initiates events that contribute to its own destruction. It is important to remember that innate immune response is only rarely able to reject an allograft on its own.
_
The figure below shows that ischemic/reperfusion injury to transplant organ activates innate immune system which activates adaptive immune system leading to acute graft rejection:
![]()
_______
In a nutshell:
Hyperacute rejection occurs due to preformed antibodies against HLA and ABO antigens, acute rejection occurs due to direct allorecognition of non-self HLA antigens and chronic rejection occurs due to indirect allorecognition of non-self HLA antigens.
_____
Immunologic Mechanisms for transplant rejection in brief:
- The HLA system is a key factor in most reactions. Reactions are mediated by either T lymphocytes or by antibody. The major types of hypersensitivity reactions involved are types II and IV.
- The ABO system, best characterized as the major blood group antigens, is also important because these antigens are expressed on all cells except those in the central nervous system. Thus, matching for ABO compatibility is important for transplantation.
- T-cell mediated reactions: Can be either CD4+ cells generating delayed hypersensitivity reactions after recognizing foreign HLA class II (DR) antigens or cytotoxic CD8+ cells recognizing foreign HLA class I (A,B, or C) antigens. The donor tissue or donor lymphocytes within the transplanted tissue carry the offending HLA antigens.
- Antibody mediated reactions: These can be mediated through complement-mediated cytotoxicity, antibody-dependent cytotoxicity (ADCC), or immune complexes.
_______
Clinical HLA Testing:
To support the transplant programs, several clinical laboratories perform various HLA tests, including HLA typing of the recipient and the donor, screening of HLA antibodies in the recipient, and detection of antibodies in the recipient that are reactive with lymphocytes of a prospective donor (cross-matching).
Historically, HLA typing was conducted by serologic testing by using antiserum in complement-dependent cytotoxic assays. Recently, more precise DNA-based HLA typing methods using molecular techniques, such as sequence-specific oligonucleotide probe hybridization, sequence-specific primer amplification, sequencing-based typing, and reference strand-based conformation analysis, have been developed and are frequently used.
There is a clear relationship between the degree of HLA matching and kidney graft survival in transplants from living-related donors. Simultaneous analysis of 5,262 one haplotype-matched living-related allografts, and 973 HLA identical allografts showed 10-year projected survival rates of 52% and 73% and graft half-lives of 11.9 and 23.6 years, respectively. Conversely, the influence of HLA matching on the survival of liver and thoracic organs is yet uncertain.
To avoid hyperacute rejection, it is very important to identify recipient anti-HLA antibodies to antigens expressed on donor cells. The pioneer method to detect such antibodies, the complement-dependent cytotoxicity (CDC), has been gradually replaced by more-sensitive solid-phase assays, such as the enzyme-linked immunosorbent assay and the bead-based technology (i.e., flow cytometry: FlowPRA and Flow Analyzer: Luminex). However, the new techniques have been associated with decreased specificity, and some non-HLA antigens with no clinical relevance have been able to give a positive crossmatch. These “false-positive” antibody results have as a consequence a decreased chance of the patient to receive an organ by way of exchange organizations, thus decreasing chances for the patient. Thus, the experts recommend that the information these tests provide should complement that of the direct CDC assay.
_
HLA Compatibility:
Tissue typing of recipient and donor determines their human leukocyte antigen (HLA) match. HLA antigens are coded on chromosome 6, with half (one haplotype) inherited from each parent. The major histocompatibility class I HLA-A and HLA-B and class II HLA-DR antigens are routinely determined as rejection responses are thought to most commonly stem from mismatches at these alleles. A six-antigen (HLA-A, HLA-B, and HLA-DR from each parent) match confers a graft survival advantage compared with 0 antigen matches for both cadaveric and live donor transplantation of 10% at 10 years.
What is six-antigen match?
They are the A, B, and DR antigens. There are two antigens for each letter and they are identified by numbers. So, your HLA type might look something like this:
A2, A30
B8, B70
DR3, DR8
You inherit these from your parents, three (A, B, and DR) from your mother and three (A, B, and DR) from your father. So 3 + 3 = 6 antigen match.
In addition to determination of the HLA compatibility, cross matching and screening for anti-HLA antibodies are performed to assess the risk of rejection. There is an increasing awareness of the importance of immune responses to other HLA antigens, and many centers now look for the presence of antibodies to HLA-C, HLA-DQ, and HLA-DP. HLA‐C matching of all kidney donors and recipients may result in a better transplantation outcome.
_
It is believed that the better the HLA match, the more successful the transplant will be over a longer period of time. A parent and child would have at least a 50 percent chance of matching, siblings could have a zero to 100 percent match, and unrelated donors would be less likely to match at all. The best match for the recipient is to have 12 out of 12 antigen match i.e. HLA-A, B, C, DR, DQ and DP from each parent. (This is known as a zero mismatch seen in identical twin) It is possible albeit rare for all 12 markers to match, even with an unrelated deceased donor organ, if the patient has a very common HLA type. A kidney with a 12 antigen match rate has a 40% more chance for survival (for a 5-year-period) than a 4-6 mismatch kidney. Tissue matching is crucial in cadaveric donors or in the case of transplantation from a relative. However, in alternative transplantation cases (spouses or unrelated donors) tissue matching might not be indispensable since the patient has no other viable choice. Mismatching of MHC-II provokes more rapid and severe rejection than mismatching of MHC-I antigens.
_
The value of tissue matching for transplantation between family members has been established beyond any doubt. At the same time, the very complexity of the human histocompatibility system has militated against easy matching between nonrelated people. At a practical level, close matching for transplantation of cadaver kidneys has become less of a consideration, especially since the availability of cyclosporine. With transplantation of the liver, heart, and other extrarenal organs, tissue matching has not even been taken into consideration since the events leading to and connected with transplantation occur so quickly that a labored search for a well-matched organ is not possible. Surprisingly, good results can be obtained even with completely mismatched cadaver organs, and this fact has reduced progressive emphasis on antigen matching. However, none of the immunosuppressive measures available today can prevent the immediate destruction of transplanted kidneys by preformed humoral antibodies in a condition that has been called “hyperacute rejection.” Terasaki et al described the first example of this phenomenon in 1965, with prompt confirmation by Kissmeyer-Nielsen of Denmark and by many others. Hyperacute rejection is most commonly seen with kidney transplants, but the heart and liver (in that order of susceptibility) can also be similarly destroyed. Hyperacute rejection can be avoided by the so-called crossmatch test, which detects anti-donor antibodies in the recipient’s serum before the procedure. Crossmatching has proved to be the single most important practical contribution of tissue typers to the practice of transplantation during the last quarter century.
_
In classical serological HLA testing, antibodies are used to distinguish between different variants of HLA antigens. Each antibody is specific for a particular antigen, and by using different antibodies HLA serotyping is performed to determine if the donor serotype is a good match for the recipient. However, serological testing is limited by the number of antibodies available against specific HLA antigens. More recently, molecular techniques have been used for HLA DNA typing; these are superior to classical serological tests. The HLA Class I genes are by far the most polymorphic genes in the human genome. Current molecular techniques for HLA DNA typing include recombinant DNA technology, chain-termination Sanger sequencing, and polymerase chain reaction (PCR)-based amplification. These molecular tests can recognize more alleles than traditional serological testing.
_
Assessing HLA Sensitization:
IgG antibodies against class I (HLA-A and HLA-B) antigens are highly associated with acute rejection and are a contraindication to transplantation. IgM antibodies against HLA antigens may also predict rejection if they are present in current but not past sera; however, they may also be falsely positive. Prior treatment of sera with dithiothreitol can remove IgM antibodies and aid in the interpretation of the test. Autoantibodies (such as may occur in lupus) may also give false-positive results and can be determined by prior absorption with autologous lymphocytes. Sensitization to HLA antigens generally occurs through blood transfusion, pregnancy, or prior transplantation. Presence in the recipient of antibodies to donor-specific HLA antigens can result in hyperacute rejection. Crossmatching of donor lymphocytes with recipient serum allows screening for this possibility. Terasaki and coworkers pioneered the complement-dependent cytotoxicity (CDC) crossmatch. This assay determines the presence of antibodies thought to be of clinical significance by mixing donor T or B lymphocytes with recipient serum in the presence of complement. The sensitivity of the assay can be augmented by the addition of anti-human globulin. Presence of a positive T-cell CDC crossmatch to the donor is highly predictive of hyperacute rejection, whereas a B-cell CDC crossmatch is more subject to false-positives but should prompt a search for donor-specific antibodies. A positive T-cell crossmatch is an absolute contraindication to transplantation. The flow crossmatch is more sensitive than the CDC in detecting antibody capable of binding to donor T or B lymphocytes. Binding of antibody from donor serum is detected by flow cytometry after probing with a fluorescein-labeled anti-immunoglobulin antibody. The predictive value of a positive flow crossmatch for rejection is less than that of a CDC crossmatch because of its increased sensitivity, and it does not assess the ability of the antibody to fix complement. In most centers, it is not routinely performed before cadaveric donor transplants, but it is commonly performed in a live donor transplant workup. A positive flow crossmatch (with a negative CDC crossmatch) is not an absolute contraindication to proceeding; however, it may lead the team to alter the immunosuppressive regimen (e.g., desensitization protocol) to decrease the risk or severity of antibody-mediated rejection.
Determination of the presence of anti-HLA antibodies in the recipient’s serum is increasingly used as a means of predicting rejection. This virtual crossmatch compares the specificity of the antibodies identified with the prospective donor’s HLA typing. Single-antigen bead testing, which is used to detect anti-HLA antibodies, is the final step in the current techniques used to identify antibodies that can injure the allograft. It is currently used to monitor transplant recipients and used as a diagnostic tool for AMR. There was a higher incidence of AMR in patients with pre-transplant DSA despite a negative CDC crossmatch. However, pre-transplant DSA detected by micro-bead based test had no statistically significant impact on delayed graft function, patient survival and graft survival. As well as through panel reactive antibody testing, antibodies can be detected by enzyme-linked immunosorbent assay or more sensitive antigen-coated bead technology (Luminex). Beads are coated with a single HLA antigen and are mixed with recipient serum and probed with a fluorescein-labelled anti-immunoglobulin antibody. Beads that bind antibody are therefore identified by fluorescence. The decision on whether to proceed with transplantation in the context of this information is complex.
_
What is Panel Reactive Antibody (PRA)?
This is another term you will hear often while being evaluated for a transplant. When you are exposed to foreign tissues, either through a blood transfusion, pregnancy or previous transplant, you may develop an antibody to different HLA proteins. If you test positive for HLA antibodies, you are considered “sensitized” and your PRA percentage will be greater than 0. The more HLA antibodies that you have in your blood, the higher the PRA percentage. It is important to test for the presence of these HLA antibodies before your transplant. If you have a high level of HLA antibodies, it may be more difficult to find a compatible kidney for you. However, new procedures such as plasmapheresis may be able to reduce the antibodies in your blood. As mentioned above, HLA antibodies can vary over time and so your %PRA can also change.
_
In a nutshell:
HLA typing along with ABO (blood group) typing is used to evaluate tissue compatibility between a donor and a potential transplant recipient. HLA typing is performed before various transplant procedures, including those for kidneys, liver, heart, pancreas, and bone marrow. The success of a transplant increases with the number of identical HLA antigens between a recipient and a potential donor.
Major types of HLA testing include:
- HLA antigen typing between donor and recipient: Classically this type of testing is done using serological markers, but more recently molecular (DNA) typing (which provides more information) is replacing classical serological testing.
- HLA antibody screening: Performed on the recipient in order to determine if there is any antibody present that might target donor organs, which would trigger organ rejection. HLA antibody is not always present in an individual unless the person has received a blood transfusion or is a woman post-pregnancy.
- Lymphocyte cross-matching: This step takes place when a donor is identified; the objective is to identify any antibody that, if present in the recipient, might be directed against antigens present on the donor’s lymphocyte. In this test, serum from the intended recipient is mixed with T and B lymphocytes (white blood cells) from the donor to investigate potential reactions (a positive test result) that might destroy white blood cells of the recipient.
_____
Usefulness of HLA typing in clinical organ and tissue transplantation:
Although typing for intra-familial transplants of all types is clearly of great value, the usefulness of HLA typing in cadaveric kidney grafting has been a point of controversy since cyclosporine became available. Although short term survival rates did not appear to be that different for closely or poorly matched cadaveric kidneys, the degree of HLA matching does correlate with long-term survival. Until 1980, only HLA-identical siblings could be used as bone marrow donors, because both graft rejection and lethal graft-versus-host disease (GVHD) were common complications if this was not the case. Fortunately, the development during the past 3 decades of techniques to rigorously deplete post-thymic T cells from donor marrow has permitted numerous successful half-HLA matched marrow transplants with no or minimal GVHD.
HLA matching has had the greatest clinical impact in kidney and bone marrow transplantation, where efforts are made to match at the HLA-A, -B, and -DR loci. In heart and lung transplantation, although studies have shown it would be an advantage to match especially at the DR locus, practical considerations (ischemic times, availability of donors, clinical need of recipients) make this less of a consideration. Corneal grafts are not usually influenced by HLA matching, unless being transplanted into a vascularized (or inflamed) bed.
_
HLA matching and kidney transplantation: beyond graft survival, 2013 study:
Analysis of data from the international Collaborative Transplant Study has revealed striking relationships between human leukocyte antigen mismatching and graft survival, the incidence of death from cardiovascular disease or infection, the occurrence of non-Hodgkin lymphoma, and onset of post-transplant osteoporosis and bone fracture following kidney transplantation from a deceased donor.
_____
ABO system in ODT:
Histo-blood group ABO system transferase is an enzyme with glycosyltransferase activity, which is encoded by the ABO gene in humans. It is ubiquitously expressed in many tissues and cell types. ABO determines the ABO blood group of an individual by modifying the oligosaccharides on cell surface glycoproteins. Variations in the sequence of the protein between individuals determine the type of modification and the blood group. The ABO gene resides on chromosome 9 at the band 9q34.2 and contains 7 exons. The ABO locus encodes three alleles. There are six common alleles in individuals of European descent. Nearly every living human’s phenotype for the ABO gene is some combination of just these six alleles:
A
A101 (A1)
A201 (A2)
B
B101 (B1)
O
O01 (O1)
O02 (O1v)
O03 (O2)
Many rare variants of these alleles have been found in human populations around the world.
_
The ABO blood group system is used to denote the presence of one, both, or neither of the A and B antigens on erythrocytes. A very rare (in modern medicine) mismatch in this, or any other serotype, can cause a serious, potentially fatal, adverse reaction after a transfusion, or adverse immune response to an organ transplant. The ABO system is clinically important in two aspects of solid-organ transplantation: first, as a transplantation antigen that influences graft survival, and second as an antigen-antibody system implicated in immune hemolytic anemias in ABO non-identical organ transplant recipients. Organ recipients should receive a graft that is ABO compatible. ABO grouping is still the primary test for organ donation and transplantation. The first and foremost step in graft rejection is the binding of anti-A and anti-B antibodies to the endothelial cells. This leads to initiation of cycle of complement fixation, vascular damage, and thrombosis that leads to ischemia and rejection.
_
Humans naturally have antibodies to the blood group antigens their own cells lack. These antibodies are responsible for causing serious (and sometimes fatal) reactions when they attack their targets. Since people with type A cells have antibodies to type B glycoproteins, a donor with type B blood is not compatible with a type A recipient. Similarly, those with type B cells have antibodies to type A glycoproteins, indicating a type A donor is not compatible with a type B recipient. Individuals with type AB cells lack antibodies to these glycoproteins and are therefore compatible with any potential donors (with regard to blood type matching). Those with type O have antibodies against both type A and type B cells and therefore require type O kidney donors. Thus, the person with blood type AB is the universal kidney recipient and the person with blood type O is the universal kidney donor. The Rh antigen does not function as a “transplantation antigen,” because it is only present on the surface of red blood cells and not on the parenchymal cells of the graft. The positive or negative Rh factor in the blood group does not matter for a kidney transplant. For example, someone who is blood group A positive can donate to someone who is A negative.
_
ABO incompatibility does not cause stimulation in mixed leukocyte cultures, indicating that ABO compatibility is of much less importance than HLA compatibility in graft survival. However, ABO incompatibility can result in hyperacute rejection of primarily vascularized grafts, such as kidney and heart. This is thought to occur because (1) ABO blood group antigens are highly expressed on kidney and cardiac grafts, particularly those from patients who are blood group A or B antigen secretors, and (2) preformed naturally occurring antibodies to blood group substances are present in mismatched recipients. Successful transplantation of kidneys and hearts across ABO lines has been accomplished by removing ABO antibodies in the recipient or by taking advantage of the variable expression of ABO antigens such as in A2 individuals or neonates. In general, ABO-incompatible organs are avoided in kidney and heart transplantation. ABO major mismatch liver allografts are used in 6.9% of pediatric and 2.4% of adult liver recipients due to organ shortages. Liver allografts are felt to be resistant to hyperacute rejection when transplanted across ABO barriers although reports of hyperacute rejection do exist. ABO-incompatible liver transplants are commonly associated with acute graft failure with a 46% graft failure rate reported within 30 days of the transplant. Plasmapheresis to remove recipient isohemagglutinins and/or splenectomy may be of benefit. Currently, ABO-incompatible liver allografts are reserved for patients with fulminant liver failure in whom death is imminent without transplantation and when an ABO-compatible organ is not available. ABO compatible but non-identical (minor mismatch) liver transplants are associated with modest reductions in 1- and 3-yr survival. Advances in immunosuppressive therapies to prevent immune rejection of the graft have more recently allowed performing organ transplants across the ABO barrier.
_
Concept of passenger lymphocytes in organ transplants:
The incidence of passenger lymphocyte syndrome is highest in the non-group O recipients when they are transplanted organs from group O donors. There is a restriction on the use of group O deceased-donor organs for non-group O patients in many countries. But the reverse situation has also been studied. The favorable outcome of A2 to O group liver grafting, with a patient survival of 10/10 and graft survival of 8/10, makes it possible to consider this blood group combination in non-urgent liver transplants. In transplant recipients, receiving an ABO-unmatched organ, the patient develops IgG antibodies from lymphocytes transplanted along with the graft. Passenger lymphocytes transplanted with the donor organ are capable of producing ABO antibodies and hemolysis in ABO mismatched organ recipients. Although in general, red cell antibodies do not pose major problems in cardiac transplant patients, these patients have the highest risk for passenger lymphocyte syndrome (PLS) and post-transplant hemolysis occurs in 2–5%. The patient’s direct antiglobulin test becomes reactive 1–2 weeks after transplantation. These antibodies produce sudden marked hemolysis and the antibodies typically persist for a few weeks. Passive hemolysis most frequently occurs after heart transplantation, followed by liver transplantation, kidney transplants and is rare after visceral transplants. In case of hemoglobin decrease after transplantation, hemolysis due to passive lymphocyte syndrome should be considered primarily. Immunoglobulin allotyping proved that these antibodies are of donor origin and are not patient autoantibodies. This phenomenon emerged more after azathioprine was replaced by cyclosporine for immunosuppression. Cyclosporine is more permissive for secondary antibody responses. It has occurred with tacrolimus as well. Use of aprotinin in transplant patients significantly lower (60%) blood loss and PRBC transfusion volume when compared with control subjects.
_
ABO-incompatible transplants:
Because very young children (generally under 12 months, but often as old as 24 months) do not have a well-developed immune system, it is possible for them to receive organs from otherwise incompatible donors. This is known as ABO-incompatible (ABOi) transplantation. Graft survival and mortality is approximately the same between ABOi and ABO-compatible (ABOc) recipients. While focus has been on infant heart transplants, the principles generally apply to other forms of solid organ transplantation. The most important factors are that the recipient have not produced isohemagglutinins, and that they have low levels of T cell-independent antigens. United Network for Organ Sharing (UNOS) regulations allow for ABOi transplantation in children under two years of age if isohemagglutinin titers are 1:4 or below, and if there is no matching ABOc recipient. A study found that ABO-incompatible heart transplantation during infancy results in development of B-cell tolerance to donor blood group A and B antigens. Tolerance in this setting occurs by elimination of donor-reactive B lymphocytes and may be dependent upon persistence of some degree of antigen expression. These findings suggest that intentional exposure to non-self A and B antigens may prolong the window of opportunity for ABO-incompatible transplantation, and have profound implications for clinical research on tolerance induction to T-independent antigens relevant to xenotransplantation. Limited success has been achieved in ABO-incompatible heart transplants in adults, though this requires that the adult recipients have low levels of anti-A or anti-B antibodies. Kidney transplantation is more successful, with similar long-term graft survival rates to ABOc transplants.
_
Excellent Long‐term Outcome of ABO‐Incompatible Living Donor Kidney Transplantation in Japan, 2004 study:
Owing to the severe shortage of cadaveric grafts in Japan, authors have performed ABO‐incompatible living donor kidney transplantation since 1989. This study assessed short‐ and long‐term outcomes in 441 patients who received ABO‐incompatible living donor kidney transplants between January 1989 and December 2001. They compared their results with historical data from 1055 recipients of living kidney transplantation. Overall patient survival rates 1, 3, 5, 7, and 9 years after ABO‐incompatible transplantation were 93%, 89%, 87%, 85%, and 84%, respectively. Corresponding overall graft survival rates were 84%, 80%, 71%, 65%, and 59%. The graft survival rate at 1 year in the historical controls was slightly but not significantly higher than that in recipients of ABO‐incompatible transplants. Authors conclude that long‐term outcome in recipients of ABO‐incompatible living kidneys is excellent. Transplantation of ABO‐incompatible kidneys from living donors is a radical, but effective treatment for end‐stage renal disease.
_
ABO incompatible kidney transplantation has become a routine procedure with death-censored graft survival rates comparable to the rates in compatible transplantations. Desensitization is usually achieved by apheresis and B cell-depleting therapies that are accompanied by powerful immunosuppression. These strategies are intended to deplete the level of preexisting antibodies to blood groups or to HLA antigens in the recipient and to make the crossmatch result negative. In the rituximab era, the blood type barrier can be crossed to achieve adult ABO-incompatible living donor liver transplantation (LDLT) with survival rates comparable to those of ABO-compatible LDLT, but with more biliary complications.
________
________
Tissue tolerance:
Rejection cannot be completely prevented; however, a degree of immune tolerance to the transplant does develop. Several concepts have been postulated to explain the development of partial tolerance. They include clonal deletion and the development of anergy in donor specific lymphocytes, development of suppressor lymphocytes, or factors that down-regulate the immune response against the graft. Other hypotheses include the persistence of donor-derived dendritic cells in the recipient that promote an immunologically mediated chimeric state between the recipient and the transplanted organ.
_
The immune system is more than a “seek-and-destroy” mechanism. Certain aspects of the immune system are responsible for suppressing inflammation and inhibiting the tissue destruction caused by activated T-cells. These inhibitory components of the immune system are known as T regulatory, or Treg cells. Treg cells are the counterbalance to aggressive, activated T-cells. Without Treg cells, our immune system would constantly attack our own tissue. In fact, the role of Treg cells in suppressing autoimmune diseases (e.g. diseases in which the immune system attacks the body’s own tissue, like rheumatoid arthritis, lupus, Crohn’s disease, psoriasis, etc.) has been well documented (Walker, 2008). Treg cells are critical to the tolerance of an allograft. The more Treg cells present in circulation, the weaker the attack against the transplanted tissue (Demirkiran, 2006). Ironically, the same inflammatory cytokines that stimulate aggressive T-cells also suppress Treg cells, promoting the attack against the transplanted tissue from two angles. The inflammatory cytokines IL-1β, IL-2, IL-6, IL-15, IL-21 and TNFα, by inhibiting the function of Treg cells and promoting the activation of cytotoxic T-cells, are responsible for the intensity of the attack against the transplanted tissue by the host’s immune system (Hanidziar, 2010).
_
Treg cells and T-cells originate in the thymus, a specialized organ located just behind the sternum, between the lungs. Here, non-functional progenitor cells develop (differentiate) into either the immunomodulatory Treg cells, or the aggressive cytotoxic T-cells, depending on cytokine exposure. Exposure to high levels of the inflammatory cytokines Il-1β, IL-6, or IL-21 causes progenitor cells to develop into aggressive T-cells, while exposure to sufficient levels of a highly specialized anti-inflammatory cytokine, called transforming growth factor-β (TGFβ), induces differentiation into Treg cells. Significantly, it has been shown that high levels of IL-6 inhibit the ability of TGFβ to effectively induce differentiation of progenitor cells to Treg cells, leading to an increase in the number of allograft-destroying cytotoxic T-cells. (Kimura, 2010; Hanidziar, 2010). One of the most effective strategies for modulating an over-aggressive immune response against transplanted tissue is to target the specific inflammatory cytokines that are dually responsible for the stimulation of aggressive T-cells and the suppression of protective Treg cells.
______
______
Donor and Recipient Matching in ODT:
_
Understanding Transplant Compatibility:
The ultimate goal of matching a donor kidney with the person seeking transplantation is identification of an organ that will be tolerated indefinitely by the body of the recipient (who takes medications to prevent rejection). It is helpful to divide donor and recipient matching into three distinct areas: blood type matching, tissue type matching and cross matching. Each is a distinct and important aspect of donor and recipient matching for which specific, complex laboratory tests have evolved. Each applies to kidneys from both live and deceased donors. Rejection can be minimised by carefully matching the donor and recipient for compatibility prior to transplantation. The better matched the donor and recipient are the more successful the transplantation is likely to be. Compatibility between donor and recipient is assessed using a combination of tests. Testing is also conducted for potentially transmissible diseases, such as HIV (human immunodeficiency virus), hepatitis and CMV (cytomegalovirus).
_
What tests will I need before my transplant?
Before you can be considered for an organ transplant, you will need to have medical tests to find out whether you are a good transplant candidate and to find out your tissue type. Knowing your blood and tissue type will make matching with a donor organ easier. Some tests are required for all organ transplant candidates. Other tests are needed to monitor your chronic disease or the cause of your organ failure. In general, tests that are done for all organ transplant candidates include:
- A cross-match for transplant. This blood test shows whether your body will reject the donor organ immediately. It will mix a donor’s lymphocytes with your serum to see whether your antibodies attack the antigens of the donor.
- Antibody screen. A panel-reactive antibody (PRA) test measures whether you have antibodies against a broad range of people. And if you do, it means you are at higher risk of having rejection, even if the cross-match shows that you and the donor are a good match.
- Blood type. This blood test shows which type of blood you have. Your blood type should be compatible with the organ donor’s blood type. But sometimes it’s possible to transplant an organ from a donor with a different blood type.
- Tissue type. This blood test shows the genetic makeup of your body’s cells. We inherit three different kinds of genetic markers from our mothers and three from our fathers (6 antigen HLA typing). Tissue type sometimes plays a role in matching an organ recipient to a donor.
- A mental health assessment. This test identifies any psychological issues that may prevent you from receiving and caring for your new organ. A living donor may also be required to have this test before donating an organ.
The results of these medical tests will be used to match you with an organ donor. The most important matches are for blood type, cross-match, and antibody screen.
_
When matching organs from deceased donors to patients on the waiting list, many of the factors taken into consideration are the same for all organs. These usually include:
- Blood type
- Body size
- Severity of patient’s medical condition
- Distance between the donor’s hospital and the patient’s hospital
- The patient’s waiting time
- Whether the patient is available (for example, whether the patient can be contacted and has no current infection or other temporary reason that transplant cannot take place)
Depending on the organ, however, some factors become more important. For example, some organs can survive outside the body longer than others. So the distance between the donor’s hospital and the potential recipient’s hospital must be taken into consideration.
_
The Matching Process by Organ type:
People waiting for a heart transplant are assigned a status code, which indicates how urgently they need a heart. Because organs such as the heart and lungs can survive outside the body for only 4 to 6 hours, they are given first to people who live near the hospital where organs are recovered from the donor. If no one near the donor is a match for the heart, the transplant team starts searching progressively farther away to identify a recipient. Body size also is especially important in heart matching, as the donor’s heart must fit comfortably inside the recipient’s rib cage.
The lung allocation system uses information such as lab values, test results, and disease diagnosis—to arrive at a number which represents an estimate of the urgency of a candidate’s need for transplant and the likelihood of prolonged survival following the transplant. This lung allocation score, and the common factors listed above, are considered to determine the order in which a donated lung is offered to potential recipients. Body size and distance between hospitals are especially important because lungs also must fit within the rib cage, and can survive outside the body for only 4 to 6 hours. Lungs are therefore offered first to people near the donor’s hospital. If no one near the donor is a match for the lung, the recovery team starts searching progressively farther away.
Candidates who need a liver transplant are assigned a MELD or PELD score (Model for End-Stage Liver Disease or Pediatric End-Stage Liver Disease) that indicates how urgently they need the organ. A donor liver is offered first to the candidate who matches on the above common elements and has the highest MELD or PELD score first (indicating the most need). If the first recipient’s surgeon does not accept the organ then the liver is offered to matching patients with the next highest MELD or PELD scores until the organ is accepted. Geographic factors are also taken into consideration, but livers can remain outside the body for 12 to 15 hours so they can travel farther than hearts and lungs.
The identification of potential recipients for a donor kidney involves the common elements noted above including blood type, length of time on the waiting list, whether the recipient is a child, and whether the body sizes of the donor and recipient are a good match. Other factors used to match kidneys include a negative lymphocytotoxic crossmatch and the number of HLA antigens in common between the donor and the recipient based on tissue typing, Many kidneys can stay outside the body for 24 hours so many more candidates from a wider geographic area can be considered in the kidney matching and allocation process than is the case for hearts or lungs.
When matching the donor intestine to a waiting list candidate, the ABO blood group must be identical because of the higher risk of graft-versus-host-disease (GVHD), a violent immune reaction by the lymphocytes within the donor organ against the recipient’s body that can lead to death. Also, the abdominal cavity shrinks up in many patients waiting for an intestinal transplant so the donor must usually be considerably smaller than the recipient so that the intestine will fit into the smaller space. Finally, because intestinal transplant recipients can easily get a severe infection from cytomegalovirus (CMV) and Epstein Barr virus (EBV), patients who have never been exposed to CMV or EBV before are usually matched with donors who are similarly CMV-negative or EBV-negative respectively.
______
Paired donation:
If a potential living donor is incompatible with his/her recipient, the donor could be exchanged for a compatible kidney. Kidney exchange, also known as “kidney paired donation” or “chains,” have recently gained in popularity.
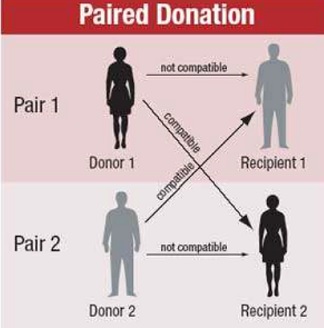
_
A “paired-exchange” is a technique of matching willing living donors to compatible recipients using serotyping. For example, a spouse may be willing to donate a kidney to their partner but cannot since there is not a biological match. The willing spouse’s kidney is donated to a matching recipient who also has an incompatible but willing spouse. The second donor must match the first recipient to complete the pair exchange. Typically the surgeries are scheduled simultaneously in case one of the donors decides to back out and the couples are kept anonymous from each other until after the transplant. Paired-donor exchanges more efficiently allocate organs and lead to more transplants.
_
Research in matching and rejection, a 2017 study:
Even when organs are chosen to have closely matching MHC proteins, subtle differences can still produce immune responses. For example, one in 10 hearts and nearly one in 20 kidneys will show signs of being rejected by the body within the first year in spite of being declared compatible. To avoid rejection, organ recipients need to be on treatments that suppress the immune system resulting in infection and cancer. Researchers have identified a previously hidden link between our immune system and the activation of cells that lead to organ rejection. The discovery opens the way for scientists to develop new forms of treatment that could prevent immune responses from attacking life-saving tissue transplants without leaving the body so open to infection or cancer. A type of receptor on bone marrow cells called signal regulatory protein alpha (SIRPα) has been identified by scientists from the University of Pittsburgh as the body’s watchdog responsible for dispatching the lymphocytes that target and destroy foreign cells. SIRPα isn’t an unknown protein, already understood to bind to another protein called CD47 that triggers a range of immune responses in different white blood cells. Joining the dots, the researchers believe CD47 on monocytes – the white blood cells that grow into dendritic cells – interact with SIRPα receptors on foreign tissues, setting off the entire ID check process. Once these cells are activated, then they turn around and activate the rest of the immune system, and that leads to the full-blown rejection of the organ. A better match between the donor’s and recipient’s SIRPα genes could help reduce the risk of the immune response being sparked in the first place. New treatments focussing on SIRPα might help reduce the doses or types of medications, and possibly help prolong the organ’s life. This research was published in Science Immunology.
_
Personalized Donor-Recipient Matching for Organ Transplantation using artificial intelligence algorithm, a 2017 study:
Organ transplants can improve the life expectancy and quality of life for the recipient but carry the risk of serious postoperative complications, such as septic shock and organ rejection. The probability of a successful transplant depends in a very subtle fashion on compatibility between the donor and the recipient – but current medical practice is short of domain knowledge regarding the complex nature of recipient donor compatibility. Hence a data-driven approach for learning compatibility has the potential for significant improvements in match quality. This paper proposes a novel system (ConfidentMatch) that is trained using data from electronic health records. ConfidentMatch predicts the success of an organ transplant (in terms of the 3-year survival rates) on the basis of clinical and demographic traits of the donor and recipient. ConfidentMatch captures the heterogeneity of the donor and recipient traits by optimally dividing the feature space into clusters and constructing different optimal predictive models to each cluster. The system controls the complexity of the learned predictive model in a way that allows for assuring more granular and accurate predictions for a larger number of potential recipient-donor pairs, thereby ensuring that predictions are “personalized” and tailored to individual characteristics to the finest possible granularity. Experiments conducted on the UNOS heart transplant dataset show the superiority of the prognostic value of ConfidentMatch to other competing benchmarks; ConfidentMatch can provide predictions of success with 95% accuracy for 5,489 patients of a total population of 9,620 patients, which corresponds to 410 more patients than the most competitive benchmark algorithm (DeepBoost).
_______
_______
Blood transfusion versus organ transplant:
There are several important differences between blood transfusions and organ transplants. Transfused red cells are expected to last for no more than three months, while transplants will hopefully function for many years. Transfusions are given intravascularly, and transplants are, of course, implanted. Immune responses to foreign antigens that are given intravascularly tend to be less pronounced than responses to antigens introduced through other routes. Transplanted organs contain some immune cells from the donor that can stimulate the recipient, whereas most immune cells that might be in a transfusion are filtered out before administration.
_
Blood transfusions may be rejected by the recipient, resulting in a transfusion reaction, but such cases are relatively rare. In order to comprehend how this can happen, it is necessary to understand some basic immunology. There are two basic types of immune responses: humoral, or antibody-mediated, and cellular. Humoral immune responses result in the production of antibodies that are specific to a foreign antigen. When these antibodies attach to the antigen–on bacteria, for example–immune complexes are formed. The body’s macrophages, mainly in the liver and spleen, then remove and destroy the immune complexes. Once attached to antigens, antibodies can also activate what is known as the complement pathway. As an end result, complement activation can punch holes in the membranes of bacteria or cells that are coated with antibodies. When red blood cells are the target of antibodies and complement, a condition called hemolysis results. Immune responses evoked by blood transfusion, when they occur, are usually humoral in nature. Organ and bone marrow transplants, in contrast, usually evoke cellular immune responses, which lead to the production of specific cytotoxic lymphocytes.
_
The most important blood cell antigens in transfusion are in the ABO system. Blood types can be A (having A but not B antigens on red cells), B (having B but not A antigens), AB (having both A and B antigens), or O (having neither). Virtually everyone over the age of six months has antibodies to the A or B antigens that they don’t produce. For example, a group A individual has A antigen on his red cells and anti-B in his plasma. If blood is transfused to a patient who already has antibodies to the transfused cells (giving this individual group B blood, for example) then a serious reaction can occur. Because antibodies to A and B antigens are good at activating complement, transfusion of ABO incompatible red cells can cause breakdown of the cells in circulation and a strong inflammatory response. The end result can be kidney failure and even death. Fortunately, this type of immediate rejection of transfused red cells is rare.
_
A more common type of rejection of transfused red cells is a delayed hemolytic reaction. In this case, the patient does not have preexisting antibodies to the transfused red cells. Rather, an immune response occurs days to weeks after the transfusion. The antibodies produced in such reactions tend not to activate complement, so the transfused red cells in circulation do not usually break down. Instead, the cells are removed by the spleen and a milder inflammatory response may occur. Delayed hemolytic reactions occur in about one out of every 5,000 transfusions. The antibodies involved can be directed against one or more of hundreds of known blood group antigens. Delayed hemolytic transfusion reactions usually are not very severe, but sometimes do cause renal failure. Patients with sickle cell anemia are at greater risk of having delayed hemolytic reactions because they often receive many transfusions. These reactions can be more severe than in other patients because the loss of normal hemoglobin containing red cells and the inflammation caused by the reaction can trigger a sickle crisis.
_
Blood banks perform pretransfusion compatibility testing to avoid hemolytic reactions. Routine pretransfusion testing consists of analyzing the patients red cells for A and B antigens, testing for the presence of anti-A and anti-B in the plasma, testing for the Rh(D) antigen on red cells and screening for other red cell antibodies in the plasma. Because ABO incompatibility can be so serious, doctors need to be sure that a patients ABO type is correct. That is why hospitals test for both the antigens and the antibodies and require agreement between the tests in order to conclude the blood type. Out of hundreds of other blood group antigens (including dozens in the Rh system), testing is routinely performed for only one other: the Rh(D) antigen, which is the most likely to cause an immune response. If it is present, the patient is Rh-positive. There is about an 85 percent chance that an Rh-negative person will make antibodies if transfused with Rh-positive blood, whereas other blood group antigens are not such strong immune stimulators. The screening test for unexpected (not A or B) antibodies covers about 25 that patients are most likely to make and can detect red cell antibodies that were generated in response to previous transfusions or pregnancies. If the screen is positive, further testing is performed to identify the specificity of the antibody and select blood from a donor that lacks the corresponding antigen. More commonly, the antibody screen is negative and we can safely transfuse ABO compatible red cells despite other blood group differences between the donor and recipient that may be present.
_
The situation is a little different for transfusions of platelets rather than red cells, which occur with patients undergoing chemotherapy. Because A and B antigens are weakly expressed on platelets, they are less important in this case. Although there are antigens that are specific to platelets, it is rare for people to make antibodies against them even after repeated transfusions. But HLA antigens, which are critically important in transplantation, are strongly expressed on platelets (but only very weakly expressed on red cells). It is common for patients to make antibodies to HLA antigens in response to transfusions or pregnancy. When platelets are transfused to a patient with corresponding HLA antibodies they are very rapidly cleared from circulation, which is essentially immediate rejection of the transfusion. Usually there is not a clinically evident reaction, as in case of incompatible red cell transfusion, but the platelet transfusion is ineffective. Such a patient can become refractory to platelet transfusion (meaning that the platelet count does not rise and the patient experiences no benefit) and may be at risk for serious bleeding. Refractoriness to platelet transfusion is a serious problem in cancer chemotherapy and bone marrow transplantation. Unfortunately, it is much more difficult to test for HLA and platelet antibodies than it is to test for red cell antibodies. Platelet compatibility testing is done for patients who do not have a successful response after several platelet transfusions.
_
Things get even more complicated when white cells (such as lymphocytes) are transfused. Normally, there are very small numbers of viable white cells in most units of blood transfused today. People with normal immune systems can reject transfused donor lymphocytes, which is a good thing. If transfused lymphocytes are not rejected there can be problems. Very sensitive tests for donor white cells have shown that they may persist in the recipients blood for one or two weeks after transfusion before they are rejected. It is possible for transfused lymphocytes to survive and proliferate, however. Small numbers of donor lymphocytes have been found in some patients months or years after transfusion. This results in a state of microchimerism, in which a little of the patient’s immune system is genetically foreign. We do not know the full implications of microchimerism, but it most likely causes some abnormalities in immune responses. In the most severe case, transfused lymphocytes not only survive, but also react against the patients tissues. This causes graft-versus-host disease, which is usually fatal. Patients with markedly impaired cellular immunity are at risk of transfusion-associated graft-versus-host disease. Blood for such patients is routinely gamma irradiated to prevent this rare but very serious reaction.
_____
_____
Sensitization:
If a person has become highly sensitized, his or her immune system is hyper-vigilant to invaders — even when the invader is a life-saving transplanted organ. Sensitization by previous pregnancies or transplants is considered unavoidable, but it is blood transfusions given to these patients that lead most often to broad sensitization. Both leukocytes and red cells carry a significant HLA antigen load, and residual leukocytes and/or red cell HLA may explain why leukocyte‐reduced units are unable to prevent sensitization to any significant degree. Prevention of sensitization will require a more active effort to avoid blood transfusions, whenever possible. When transfusions are required, there is evidence that the use of HLA‐matched blood or immunosuppression in selected situations may reduce sensitization, even in patients previously exposed to alloantigens. Sensitization continues to be a serious and difficult problem for organ transplant patients. Although the use of plasma exchanges and immunosuppression to transplant sensitized patients has a long history, only in recent years desensitization has been brought to the forefront of organ transplantation. The hallmark of these recent, more aggressive approaches to transplant sensitized patients has been a “can do” attitude, whereby expensive and cumbersome treatments with uncertain rewards were no longer an impediment to offer these patients the option of transplantation. Clearly, a similar effort has not been applied to the prevention of sensitization.
_
Although sensitization is produced by previous transplants, pregnancies or transfusions, the incidence, degree and duration of the antibody response (and therefore its clinical significance) are the result of complex interactions largely determined by the nature of the alloantigenic event and the immunologic history of the patient. Unfortunately, this complexity is often overlooked in favor of misconceptions, like erythrocytes do not express HLA antigens, transfusions induce only HLA antibodies against the transfusion donor or leukocyte‐reduced blood is the solution to transfusion‐induced sensitization.
_
HLA Molecules in Blood Transfusions:
HLA content of leukocytes:
Much of the antigen load in a blood unit is present in lymphocytes, which express between 105 and 2 × 105 class I HLA molecules per cell. Other leukocytes express less. Platelets are rich in HLA molecules, but they are routinely removed from packed red cell units. Monocytes also express class II HLA antigens (1–2 × 104 antibody–phycoerythrin molecules/monocyte).
HLA content of erythrocytes:
The HLA class I molecules in erythrocytes are expressed constitutively at low levels, and at higher levels under genetic and environmental influences. Radiolabeling techniques and Scatchard analysis show that erythrocytes contain 100–2000 class I HLA molecules per cell. Thus, the HLA content of erythrocytes is as significant as that of leukocytes because there are 1000 times more red cells than leukocytes in a blood unit. Erythrocytes from individuals positive for HLA‐B7 express more, a fact recognized long ago as responsible for the presence of the red cell antigen Bga. Erythrocyte HLA expression is also higher in patients receiving interferon alpha for viral hepatitis and in HIV infection.
_
Down‐Regulatory Effects of Blood Transfusions:
Despite the high HLA content of blood transfusions or perhaps because of it, transfusions do not often elicit an antibody response in naive recipients. In fact, they are immune down‐regulatory, as shown by the “transfusion effect” of improved renal graft survival when patients received either random donor or donor‐specific transfusions (DSTs). Multiple clinical and experimental studies have implicated induction of anergy, inhibitory cytokines, regulatory T cells and other mechanisms triggered by the intravenous administration of alloantigens, as mechanisms involved in this phenomenon. The immune modulating effect of transfusions seems to be also responsible for an increased rate of infections in patients with trauma or burns. Improved transplant outcomes were seen in transfused patients during the 1970s and 1980s, when 1‐year renal graft survival was 60–70%. In the modern immunosuppression era, with 1‐year graft survival rates around 90%, this effect is less evident, possibly still present according to some reports but not according to others.
_
Sensitization by blood transfusions as the sole alloimmunogenic event:
As mentioned above, transfusions are poorly immunogenic in naive recipients. The incidence of HLA antibodies in renal transplant candidates, who had no previous pregnancies or transplants, is 10–12%, as measured by either cytotoxicity in patients who received up to 20 transfusions or enzyme immunoassay. When HLA antibodies were produced, they seldom reached high levels and decreased to baseline after a few months, even after subsequent transfusions. Furthermore, patients who became sensitized by protocol transfusions were successfully transplanted with deceased donor kidneys when antibodies declined. Although these considerations stress that clinically significant sensitization in these patients is uncommon, the potential for sensitization is always present. The practice of transfusing only when it is strictly necessary should be universal, although using prevention measures, such as immunosuppression or HLA matched blood when transfusions are unavoidable, may not have a favorable risk or cost benefit ratio in naive patients. Although the risk of sensitization by transfusions is low in naive recipients, sensitization does occur, especially in pediatric recipients and when multiple transfusions are given.
_
Contribution of Pregnancies to the Risk of Sensitization by Transfusions:
Most patients with past pregnancies and no transfusions are either weakly or not sensitized, and usually proceed to transplantation with no undue delays. In contrast, it is not uncommon to see multiparous patients with little or no HLA antibodies at presentation, who become highly sensitized by a few transfusions before or during listing.
_
Sensitization by Previous Transplants and by Previous Transplants Followed by Transfusions:
Patients, who have a functioning graft, may become sensitized while they are under immunosuppression. De novo posttransplant antibodies are a risk factor for graft rejection and graft loss, although they have also been observed in patients with stable renal function. De novo antibodies are rare early after transplantation, become more frequent with time after transplant and can be a major factor in late graft failure. Although some patients appear to make antibodies through an escape from immunosuppression, decreased immunosuppression due to noncompliance or presence of infections or posttransplant lymphoproliferative disease probably play a major role in sensitization. The incidence of sensitization in patients who lost a transplant reported in various studies is around 70%. However, most patients are not sensitized at the time of transplant loss. In a recent study of 85 patients followed after transplant loss, only 16 (19%) were sensitized at the time of graft loss. About half of the remaining patients made antibodies subsequently, possibly because of discontinuation of immunosuppression, transfusions or graft nephrectomy, for an overall rate of sensitization of 70 %. Another interesting observation was reported in two unsensitized retransplant candidates. After one or two transfusions, both patients made antibodies that were specific for the previous transplant donor but not for the blood donors, as shown by a negative crossmatch against blood donor lymphocytes. This observation and the fact that the majority of previously transplanted patients, most of them also transfused, show antibody specificity for the antigens of the transplant donor, suggests that in these cases, the transplant HLA antigens are the source of antigenic stimulation and that the transfusions represent a triggering event, either by HLA cross‐reactivity or nonspecific polyclonal B‐cell activation. Thus, patients who remain unsensitized at the time of transplant loss may still be at high risk of making broadly reactive antibodies if transfused. This point is critical for applying measures to minimize sensitization when retransplantation is an option.
_
Strategies for Prevention of Sensitization by Education and Risk Avoidance:
![]()
Although most sensitized patients had past pregnancies or transplants, the previous discussion highlight the point that high sensitization occurs almost always when blood transfusions are given after pregnancies or graft loss. Sensitization may not be avoided in all cases, but there exists the potential to reduce its incidence by applying a range of measures that target patients in specific situations.
_
Identifying patients at risk:
Because of the higher risk of patients with previous pregnancies or transplants, especially if they are already weakly sensitized, transplant teams should have protocols for identifying them and communicating with patients and their referring physicians about sensitization risk, in case transfusions are needed. Cardiac surgery in heart transplant candidates is also a risk factor, especially in children, because of the possibility of many transfusions in a short period of time.
_
Avoiding transfusions:
The use of blood transfusions in renal disease patients decreased between 1992 and 2005, but it continues to be common. The decrease can be attributed to the increased use of erythropoietin stimulating agents (ESAs) and increased awareness of transmission of infections and other untoward effects. The ESAs have risks that need to be balanced against the consequences of sensitization. Blood banks can advise regarding the collection of one or two blood units from the patient for autologous transfusions during prospective elective surgery.
_
When patients need to be transfused, using HLA‐matched blood or immunosuppression, are the options to be considered. If transfusions are needed, HLA matching may be used when there is time to procure blood units, and immunosuppression may be used for acute needs. However, there are still many questions that remain to be answered, including what is the minimum degree of matching that can be effective or if one haplotype matched relatives may be used or what are the best strategies to make matching logistically successful. Immunosuppressive protocols (drugs of choice, length and safety of treatment) need to be developed and tested in specific circumstances, such as at the time of graft loss, elective surgery or other situations, when transfusions cannot be avoided. Also, a question for future consideration is whether these measures should be applied only to patients who had previous transplants or pregnancies or be more inclusive.
_______
_______
The fetus is an allograft that is tolerated repeatedly:
All of the transplants discussed so far are artefacts of modern medical technology. However, one tissue that is repeatedly grafted and repeatedly tolerated is the mammalian fetus. The fetus carries paternal MHC and minor H antigens that differ from those of the mother, and yet a mother can successfully bear many children expressing the same non-self MHC proteins derived from the father. The mysterious lack of rejection of the fetus has puzzled generations of reproductive immunologists and no comprehensive explanation has yet emerged. One problem is that acceptance of the fetal allograft is so much the norm that it is difficult to study the mechanism that prevents rejection; if the mechanism for rejecting the fetus is rarely activated, how can one analyze the mechanisms that control it?
_
Various hypotheses have been advanced to account for the tolerance shown to the fetus. It has been proposed that the fetus is simply not recognized as foreign. There is evidence against this hypothesis, as women who have borne several children usually make antibodies directed against the father’s MHC proteins; indeed, this is the best source of antibodies for human MHC typing. However, the placenta, which is a fetus-derived tissue, seems to sequester the fetus away from the mother’s T cells. The outer layer of the placenta, the interface between fetal and maternal tissues, is the trophoblast. This does not express classical MHC class I and class II proteins, making it resistant to recognition and attack by maternal T cells. Tissues lacking class I expression are, however, vulnerable to attack by NK cells. The trophoblast might be protected from attack by NK cells by expression of a non-classical and minimally polymorphic HLA class I molecule—HLA-G. This protein has been shown to bind to the two major inhibitory NK receptors, KIR1 and KIR2, and to inhibit NK killing.
_
The placenta may also sequester the fetus from the mother’s T cells by an active mechanism of nutrient depletion. The enzyme indoleamine 2,3-dioxygenase (IDO) is expressed at a high level by cells at the maternal-fetal interface. This enzyme catabolizes, and thereby depletes, the essential amino acid tryptophan at this site. T cells starved of tryptophan show reduced responsiveness. Inhibition of IDO in pregnant mice, using the inhibitor 1-methyltryptophan, causes rapid rejection of allogeneic but not syngeneic fetuses. This supports the hypothesis that maternal T cells, alloreactive to paternal MHC proteins, may be held in check in the placenta by tryptophan depletion.
_
It is likely that fetal tolerance is a multifactorial process. The trophoblast does not act as an absolute barrier between mother and fetus, and fetal blood cells can cross the placenta and be detected in the maternal circulation, albeit in very low numbers. There is direct evidence from experiments in mice for specific T-cell tolerance against paternal MHC alloantigens. Pregnant female mice whose T cells bear a transgenic receptor specific for a paternal alloantigen showed reduced expression of this T-cell receptor during pregnancy. These same mice lost the ability to control the growth of an experimental tumor bearing the same paternal MHC alloantigen. After pregnancy, tumor growth was controlled and the level of the T-cell receptor increased. This experiment demonstrates that the maternal immune system must have been exposed to paternal MHC alloantigens, and that the immune response to these antigens was temporarily suppressed. Yet another factor that might contribute to maternal tolerance of the fetus is the secretion of cytokines at the maternal-fetal interface. Both uterine epithelium and trophoblast secrete cytokines, including transforming growth factor (TGF)-β, IL-4, and IL-10. This cytokine pattern tends to suppress TH1 responses. Induction or injection of cytokines such as interferon (IFN)-γ and IL-12, which promote TH1 responses in experimental animals, promote fetal resorption, the equivalent of spontaneous abortion in humans.
_
The fetus is thus tolerated for two main reasons: it occupies a site protected by a nonimmunogenic tissue barrier, and it promotes a local immunosuppressive response in the mother. There are several sites in the body have these characteristics and allow prolonged acceptance of foreign tissue grafts. They are usually called immunologically privileged sites. These include eyes, testes, CNS and articular cartilage. Medically, a cornea transplant takes advantage of this, and so also knee meniscal transplantation.
_____
_____
Cell Migration and Chimerism after Whole-organ Transplantation: The Basis of Graft Acceptance a 2010 study:
A genetic chimerism or chimera is a single organism composed of cells with distinct genotypes. Chimerism can occur in animals is by organ transplantation, giving one individual tissues that developed from a different genome. Improvements in the prevention or control of rejection of the kidney and liver have been largely interchangeable and then applicable, with very little modification, to thoracic and other organs. However, the mechanism by which anti-rejection treatment permits any of these grafts to be “accepted” has been an immunological enigma. Authors have proposed that the exchange of migratory leukocytes between the transplant and the recipient with consequent long-term cellular chimerism in both is the basis for acceptance of all whole-organ allografts and xenografts.
The first unequivocal evidence that whole-organ grafts in human beings become genetic composites (chimeras) was obtained in 1969 with karyotyping studies in female recipients of livers obtained from male cadaveric donors. Postoperatively, the hepatocytes and the endothelium of the major blood vessels of the grafts retained their donor sex, whereas the entire macrophage system, including the Kupffer cells, was replaced with recipient female cells (identified by their characteristic Barr bodies) within 100 days (Figure below, middle). These observations attracted considerable attention at the time, primarily because of their implication that liver-based inborn errors of metabolism could be corrected permanently by liver replacement. This prediction has been met since then in nearly two dozen such heritable diseases. Each report of another liver-based metabolic disorder that was corrected by liver replacement added to the illusion that the composite (chimeric) structure of the hepatic allograft was a special feature of this organ.
_
Successful transplants were long envisioned as an alien patch in a homogeneous host (Figure below, left).
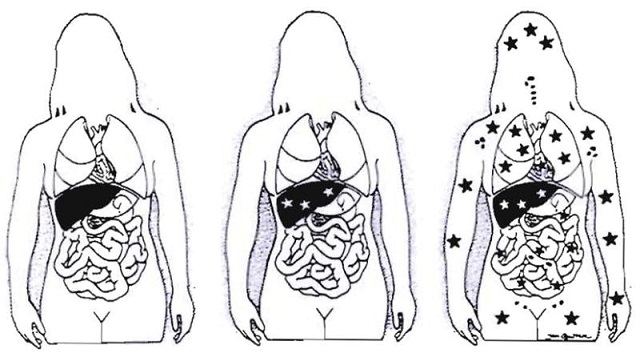
Figure above shows steps in understanding liver transplantation: left– historical view; middle – realization in 1969 that the liver graft became a genetic composite (chimera); right–proof in 1992 of systemic chimerism. Stars represent cell exchange between graft and host.
_
The illusion of uniqueness of the hepatic graft was dispelled in 1991 with the demonstration, first in rat models and then in human beings, that all successfully transplanted intestines also were chimeric. The epithelium of the bowel remained that of the donor, but lymphoid, dendritic and other leukocytes of recipient phenotype quickly became the dominant cells in the lamina propria, Peyer’s patches and mesenteric nodes. The transformation in experimental animals and in human beings was the same whether the bowel was transplanted alone or as a part of a multivisceral graft that also contained the liver, stomach and pancreas. As with that of the liver graft before it, the chimerism of the intestinal graft was made easier to demonstrate by the large constituency of lymphoreticular cells of the normal bowel. An additional crucial factor was the increasing sophistication of cell phenotyping techniques with which to differentiate donor from recipient cells in either experimental animals or human beings. For the first time, it was speculated in 1991 that graft chimerism might be a generic feature of all accepted grafts. This speculation soon was demonstrated with the kidney and thoracic organs. Later on systemic chimerism was recognised.
______
______
Various organs and tissues transplanted:
_
Transplantable organs and tissues:
Chest:
- Heart (deceased-donor only)
- Lung (deceased-donor and living-related lung transplantation)
- Heart/Lung (deceased-donor and domino transplant)
Abdomen:
- Kidney (deceased-donor and living-donor)
- Liver (deceased-donor and living-donor)
- Pancreas (deceased-donor and living donor)
- Intestine (deceased-donor and living-donor)
- Stomach (deceased-donor only)
- Testis (deceased-donor and living-donor)
Tissues, cells and fluids:
- Hand (deceased-donor only)
- Cornea (deceased-donor only)
- Skin, including face replant (autograft) and face transplant (extremely rare)
- Islets of Langerhans (pancreas islet cells) (deceased-donor and living-donor)
- Bone marrow/Adult stem cell (living-donor and autograft)
- Blood transfusion/Blood Parts Transfusion (living-donor and autograft)
- Blood Vessels (autograft and deceased-donor)
- Heart Valve (deceased-donor, living-donor i.e. the explanted hearts of transplant recipients, and xenograft [porcine/bovine])
- Bone (deceased-donor and living-donor)
____
Kidney transplant:
A kidney transplant is a surgical procedure to place a healthy kidney from a live or deceased donor into a person whose kidneys no longer function properly. The kidneys are two bean-shaped organs located on either side of the spine just below the rib cage. Each one is about the size of a fist. Their main function is to filter and remove excess waste, minerals and fluid from the blood by producing urine. When your kidneys lose this filtering ability, harmful levels of fluid and waste accumulate in your body, which can raise your blood pressure and result in kidney failure (end-stage renal disease, which is also known as end-stage kidney disease). End-stage renal disease occurs when the kidneys have lost about 90 percent of their ability to function normally.
_
A successful transplantation, across a positive crossmatch barrier, is one of the most persistent long-standing problems in the field of kidney transplant medicine. Kidneys can also be stored longer than other organs, permitting transport to a matched recipient. Kidney, pancreas and BMT must be HLA matched at the HLA-A, -B, and -DR loci which improves the life of the transplant. The recent availability of specific anti-A or anti-B immunoadsorption columns (Glycosorb) and the use of anti-CD20 monoclonal antibody (rituximab) in different immunosuppressive regimens resulted in the introduction of ABO-incompatible renal transplantation as a routine procedure in different European countries, mainly in Sweden and Germany without splenectomy. The immunosuppressive regimen consisted of one dose of rituximab (375 mg/m2) given 2–4 weeks before immunoadsorption, followed by a conventional triple-drug immunosuppression consisting of tacrolimus, mycophenolate mofetil and prednisolone, starting 1 week before immunoadsorption. Preoperatively, anti-A or anti-B antibodies were removed using the Glycosorb ABO column, a low-molecular carbohydrate column with A or B blood group antigen linked to a sepharose matrix. Immunoadsorption with Glycosorb columns is very effective, and IgG and IgM isoagglutinin titers can be reduced by two to three titer steps with every immunoadsorption session. Similar results have been found by American and Japanese workers too. With the growing immune-manipulation of the recipient, survival rates can be raised considerably, although they remain significantly inferior to those of ABO-compatible transplantation. Data from the Collaborative Transplant Study indicate a 1-year graft survival rate of approximately 50–60% following cadaveric ABO-incompatible kidney, liver or heart transplantation, compared with 70–80% for an ABO-compatible organ.
_
Common causes of end-stage renal disease include:
- Diabetes
- Chronic, uncontrolled high blood pressure
- Chronic glomerulonephritis — an inflammation and eventual scarring of the tiny filters within your kidneys (glomeruli)
- Polycystic kidney disease
People with end-stage renal disease need to have waste removed from their bloodstream via a machine (dialysis) or a kidney transplant to stay alive. A kidney transplant is often the treatment of choice for kidney failure compared to a lifetime on dialysis. A kidney transplant can treat chronic kidney disease with glomerular filtration rate (GFR, a measure of kidney function) less than or equal to 20 ml/min and end-stage renal disease to help you feel better and live longer.
Compared to dialysis, kidney transplant is associated with:
- Better quality of life
- Lower risk of death
- Fewer dietary restrictions
- Lower treatment cost
Some people may also benefit from receiving a kidney transplant before needing to go on dialysis, a procedure known as pre-emptive kidney transplant.
But for certain people with kidney failure, a kidney transplant may be more risky than dialysis. Conditions that may prevent you from being eligible for a kidney transplant include:
- Advanced age
- Severe heart disease
- Active or recently treated cancer
- Poorly controlled mental illness
- Dementia
- Alcohol or drug abuse
- Any other factor that could affect their ability to safely undergo the procedure and take the medications needed to prevent organ rejection
HIV was at one point considered to be a complete contraindication to transplantation. There was fear that immunosuppressing someone with a depleted immune system would result in the progression of the disease. However, some research seems to suggest that immunosuppressive drugs and antiretrovirals may work synergistically to help both HIV viral loads/CD4 cell counts and prevent active rejection.
_
Sources of kidneys:
Only one donated kidney is needed to replace two failed kidneys, making living-donor kidney transplantation an option. Since medication to prevent rejection is so effective, donors do not need to be completely similar to their recipient. Most donated kidneys are procured from deceased donors. However, the use of living donors in the United States has been rising in recent years. In 2006, 47% of donated kidneys were from living donors. This varies by country: for example, only 3% of kidneys transplanted during 2006 in Spain came from living donors. In Spain, all citizens are potential organ donors in the case of their death, unless they explicitly opt out during their lifetime, but this is not the case in the US and many other countries worldwide.
_
![]()
During kidney transplant surgery, the donor kidney is placed in your lower abdomen. Blood vessels of the new kidney are attached to blood vessels in the lower part of your abdomen, just above one of your legs. The new kidney’s ureter (urine tube) is connected to your bladder. Unless they are causing complications, your own kidneys are left in place. Post-operatively, kidneys are periodically imaged by ultrasound, in order to assess the physiologic changes that often accompany transplant rejection. Imaging also allows the evaluation of supportive structures such as the anastomosed transplant artery, vein and ureter, so as to ensure they are stable in appearance. Renal function tests are also monitored. Kidney transplant recipients are discouraged from consuming grapefruit, pomegranate and green tea products. These food products are known to interact with the transplant medications, specifically tacrolimus, cyclosporin and sirolimus; the blood levels of these drugs may be increased, potentially leading to an overdose. Acute rejection occurs in 10-25% of people after the transplantation procedure is completed, during the first 60 days. Rejection does not necessarily mean the loss of the organ, but it may necessitate additional treatment and medication adjustments. The reason why kidneys fail over time after transplantation has been elucidated in recent years. Apart from recurrence of the original kidney disease, also rejection (mainly antibody-mediated rejection) and progressive scarring (multifactorial) play a decisive role. Avoiding rejection by strict medication adherence is of utmost importance to avoid failure of the kidney transplant.
_
The Benefits of Living Kidney Donation:
- Avoid the 3-5 year waiting period on the deceased donor list.
- Plan the transplant before the recipient needs dialysis as health deteriorates the longer someone remains on dialysis. Research shows that the less time a person is on dialysis, the longer a transplanted kidney will function.
- Live donor kidney lasts about 15-20 years, while the average deceased donor kidney lasts 10-15 years. Short and long term survival rates are significantly better for transplants from living donors than transplants from deceased donors.
- A kidney transplant doubles the life expectancy compared to staying on kidney dialysis treatment. There is little debate over the benefits of transplantation compared to being on kidney dialysis. Life expectancy figures comparing the two are surprising. A man between the ages of 40 – 45 could expect to live about 8 years on dialysis, if he were to receive a transplant, he could expect to live more than 20 years. Women who start dialysis between the ages of 55 – 59 could expect to live approx. 5 years. However, they could live more than 16 years with a transplant, and someone’s quality of life would improve dramatically when they are not dependent on dialysis treatments.
- The surgery can be timed for the optimal health of the recipient and for donor convenience
- Better genetic matches between donor and recipient decrease the risk of organ rejection.
- Kidneys from living donors usually work immediately, as the kidney is removed from a healthy donor and transplanted right away.
- No life expectancy changes – Donating a kidney does not affect a person’s life expectancy. On the contrary, a 1997 study concluded that people who donate a kidney have been found to outlive the average population. Twenty years after donating, 85% of kidney donors were still alive, while the expected survival rate was 66%. This phenomenon may be explained by the fact that only healthy people are approved to become donors, or perhaps donors take additional health precautions after donating a kidney.
__
The cons of living kidney donation include the following:
- Possible complications – Kidney donation is considered a low-risk procedure, but this does not mean that it is risk free. Complications occur less than 5% of the time. As with any surgical procedure, there is a small possibility of infection, anesthesia complications, bleeding, blood clots, hernias or post-operative pneumonia. These complications are often short-term and can be managed by experts.
- Possible death – The complications mentioned previously may result in the donor’s death. However, these occurrences are extremely rare. The National Kidney Registry reports that in the U.S., only 3 deaths occur out of 10,000 live donor transplants (a 0.03% mortality rate). Living liver donor mortality rate is 0.2% to 2% according to Am J Gastroenterol 2006;101:1–5
- Lifestyle changes – In preparation for kidney donation, you will be asked to make some modifications to your lifestyle to ensure your health and that of the organ you will be donating. You’ll be required to attend all your clinic visits and go through the time-consuming evaluation process, which may affect your work schedule. You’ll also need to abstain from recreational drugs and tobacco. Moderate alcohol consumption is allowed until six weeks before surgery. Donors will be able to return to all normal activities after recovery.
- Recovery and pain – After kidney transplant surgery, donors will inevitably go through a recovery period where they feel pain and discomfort. They are expected to be walking the day of surgery, and are discharged after 2 or 3 days. Kidney donors may return to work between 2 to 4 weeks after the surgery, and will gradually resume their activities.
____
Kidney-pancreas transplant:
Occasionally, the kidney is transplanted together with the pancreas. University of Minnesota surgeons Dr. Richard Lillehei and Dr. William Kelly performed the first successful simultaneous pancreas-kidney transplant in the world in 1966. This is conducted in patients who have diabetes mellitus type 1. In those patients, the diabetes is due to destruction of the beta cells of the pancreas and in whom the diabetes has caused renal failure (diabetic nephropathy). This is almost always a deceased donor transplant. Only a few living donor (partial) pancreas transplants have been conducted, though. For individuals who have diabetes and renal failure, the advantages of earlier transplant from a living donor (if available) are far superior to the risks of continued dialysis until a combined kidney and pancreas transplant procedure becomes available from a deceased donor. A patient can either receive a living kidney followed by a donor pancreas at a later date (PAK, or pancreas-after-kidney), or a combined kidney-pancreas from a donor (SKP, simultaneous kidney-pancreas). Transplanting just the islet cells from the pancreas is still in the experimental stage, but the procedure shows promise. This procedure involves taking a deceased donor pancreas, breaking it down, and extracting the islet cells that make insulin. The cells are then injected through a catheter into the recipient and they generally lodge in the liver. The recipient still needs to take immunosuppressants to avoid rejection, but no surgery is required. Most people require 2-3 such injections, and many are not completely insulin-free.
______
Liver transplant:
Liver transplantation is a surgical procedure performed to remove a diseased or injured liver and replace it with a whole or a portion of a healthy liver from another person, called the donor. Since the liver is the only organ in the body able to regenerate, a transplanted segment of a liver can grow to normal size within weeks. Liver transplantation is the only definitive treatment option for patients with irrevocable acute or chronic liver failure. In the last four decades, liver transplantation has developed from an experimental approach with a very high mortality to an almost routine procedure with good short- and long-term survival rates. Despite significant improvements in the medical management of the complications of liver cirrhosis including hepatocellular carcinoma, liver transplantation (LT) remains the only definitive treatment option for patients with end-stage liver disease. Significantly improved graft and patient survival rates have been observed over time and, in the last 15 years, are relatively stable, with an overall survival rate of 85% in the first year and ∼75% at 5 yr (Kim et al. 2013). However, ∼10% of patients listed for LT die on the waiting list (Kim et al. 2006), and many potential candidates are not listed because of the shortage of deceased donor organs. Other patients are not candidates because of comorbidities, psychosocial issues, and medical issues like hepatocellular carcinoma exceeding a designated size. Acute liver failure is less common but has an excellent outcome if the patient is transplanted promptly.
_
A living donor is usually someone in the family or a close friend. Living-donor liver transplantation in adults is a relatively new technique that evolved from the successes of living-donor liver transplantation in children and adult split-liver deceased transplantation. A healthy liver has two lobes, one is about 60 percent of the total liver and the other is 40 percent. Either lobe can be transplanted and grow into a full healthy liver for the recipient. A liver donated from a person who has died can be split and used for two recipients. A living person can donate a portion of liver and still maintain liver health. Living-donor liver transplantation allows doctors to do the transplantation without the sometimes lengthy wait for a deceased liver. Both donor and recipient livers grow to full size after the transplant.
_
During a transplant evaluation of live donation, donor safety is a primary concern. A living donor doesn’t have to be a blood relative of the recipient but the compatibility of blood types is a must. The donor must be in good health and motivated to donate for altruistic reasons. If living donation is a feasible option for the patient, a donor evaluation will be performed after the recipient’s testing is completed. After testing the donor, the transplant team decides whether the donation can be performed or not. Living donors are usually the only chance for children. Ideally, liver transplants should be performed between patients whose blood types are matching. However, in emergency cases it could also be performed between non-matching blood types to save the patient’s life. But matching of the liver sizes is a must.
_
Liver transplant procedures require maximum blood component support amongst all solid organ transplants. The liver being a highly vascular organ is prone to excessive bleeding more so in patients with portal hypertension due to ESLD. Intraoperative blood losses and transfusion requirements during adult transplantation remain difficult to predict and several studies have shown no firm conclusion in this regard. Liver transplantation is associated with considerable blood product requirement, yet bloodless transplantation has been achieved in Jehovah’s Witness patients. Currently the five issues that are challenging the clinical practice of liver transplantation and relevant to gastroenterologists are living donor liver transplantation (LDLT), recurrent viral hepatitis, non-heart-beating donors, hepatocellular carcinoma, and ABO- incompatible liver transplantation. Living donor and non-heart-beating donor transplantations were initiated as a solution to increase the donor organ pool and it is expected that there will be an increase in the number of these donors. Data from the Collaborative Transplant Study indicate a 1-year graft survival rate of approximately 50–60% following cadaveric ABO-incompatible liver or heart transplantation, compared with 70–80% for an ABO-compatible organ. The results for infants and young children are much better than those of adults, particularly for liver and heart transplantations. Data suggest that B-cell tolerance can develop in the infant age group. HLA matching is not required for liver transplants and so not done in centers worldwide. Preoperative plasmapheresis, immunoadsorption, or splenectomies are still being considered at some centers but some studies have shown excellent results even without these practices. ATG interferes with T-cell dependent activation of alloreactive B-cells by removing CD4 + T helper cells. It has been shown to trigger apoptosis not only in T-cells but also in B-cells and may thus be more effective than rituximab. Important variables affecting transfusion requirements include the severity of disease (Child’s classification), preoperative PT, history of abdominal operations, and factor V levels. Other factors identified as independent predictors of transfusion include the preoperative hematocrit value, use of the piggyback transplantation method, and operative time.
______
Heart transplant:
Heart transplants are now routine. However, the first human-to-human heart transplant in 1967 by Professor Christiaan Barnard in South Africa was big news. Few people knew that the operation was the culmination of more than 60 years of preparatory animal research. In 1912, French surgeon Alexis Carrel received a Nobel Prize for his technique for joining up blood vessels – a skill he had honed by taking embroidery lessons and practised by stitching together pieces of paper. Animal studies between 1930 and 1950 illuminated ways to beat the problems of rejection. US surgeon Norman Shumway, who had been expected to perform the world’s first human to human transplant, began transplanting hearts in dogs in the 1950s and described this preliminary work in more than 20 papers published by 1967. Barnard and his colleagues carried out nearly 50 animal heart transplants over four years in preparation for the historic operation in that year. Heart-lung transplants were later developed using monkeys. In the 12 months from April 2005 to March 2006, 154 heart transplants and 15 heart-lung transplants were carried out in the UK alone.
_
A heart transplant, or a cardiac transplant, is a surgical transplant procedure performed on patients with end-stage heart failure or severe coronary artery disease when other medical or surgical treatments have failed. As of 2016, the most common procedure is to take a functioning heart, with or without transplanting one or both lungs at the same time, from a recently deceased organ donor (brain death is the standard) and implanting it into the patient. A donated heart can only remain outside of the body for about four hours before it must be transplanted. The patient’s own heart is either removed and replaced with the donor heart (orthotopic procedure) or, much less commonly, the recipient’s diseased heart is left in place to support the donor heart (heterotopic, or “piggyback,” transplant procedure). Approximately 3500 heart transplants are performed every year in the world, more than half of which occur in the US. Post-operation survival periods average 15 years. Heart transplantation is not considered to be a cure for heart disease, but a life-saving treatment intended to improve the quality of life for recipients.
_
Heart transplants are now the third most common organ transplant operation in the U.S. Primary cardiac transplant without prior cardiac surgery poses hardly any problems of alloimmunisation toward HLA or red cell antigens. After prior coronary artery bypass surgery, leucocyte antibodies have been found in 10–15% and red cell antibodies in 3–5% of patients. Heart transplantation requires similar transfusion support as coronary artery bypass surgery. In primary transplants, 0–2 units of red cells are required. Twice this amount is generally needed when there has been prior surgery. In particular, patients who have left ventricular assist devices (LVADs) implanted as a bridge to transplantation need multiple blood components and approximately 30% develop HLA antibodies, reducing the chance of a cross-match-negative graft. DR-shared heart transplants have a better outcome than DR-mismatched grafts.
_
Complications:
Post-operative complications include infection, sepsis, organ rejection, as well as the side-effects of the immunosuppressive medication. Since the transplanted heart originates from another organism, the recipient’s immune system typically attempts to reject it. The risk of rejection never fully goes away, and the patient will be on immunosuppressive drugs for the rest of his or her life, but these may cause unwanted side effects, such as increased likelihood of infections or development of certain cancers. Recipients can acquire kidney disease from a heart transplant due to side effects of immunosuppressant medications. After transplant, it’s possible the walls of the arteries in donor heart (coronary arteries) could thicken and harden, leading to cardiac allograft vasculopathy (CAV). Surgery death rate is 5-10% in 2011.
Prognosis:
The prognosis for heart transplant patients following orthotopic procedure has increased over the past 20 years, and as of June 5, 2009, the survival rates were:
1 year: 88.0% (males), 86.2% (females)
3 years: 79.3% (males), 77.2% (females)
5 years: 73.2% (males), 69.0% (females)
In 2007, researchers from the Johns Hopkins University School of Medicine discovered that “men receiving female hearts had a 15% increase in the risk of adjusted cumulative mortality” over five years compared to men receiving male hearts. Survival rates for women did not significantly differ based on male or female donors.
______
Lung Transplant:
Healthy person breaths at least 12 to 14 times per minute removing carbon dioxide from the blood and exchanging it with oxygen. While a person can live a normal life with only 30 percent of lung function; Lung transplants are recommended for those with severe lung disease, such as cystic fibrosis and COPD (chronic obstructive pulmonary disease). Patients on the lung transplant waiting list are often severely disabled and might even require oxygen 24-hours-a-day. This is why it is crucial for these individuals to receive a transplant in a timely fashion. Living lung donation is a possibility in rare cases, as two living donors can each offer a lobe their lungs, which are then both transplanted into the patient.
- The most common type of lung transplant is a single lung transplant.
- More than 1,700 patients await lung transplants in the U.S.
- Lungs are allocated to patients based on several factors including distance from donor, medical condition, and age (lungs from pediatric and adolescent donors are offered first to pediatric and adolescent patients).
______
Pancreas Transplant:
Problems with the pancreas can lead to many health problems. These include pancreatitis, or inflammation of the pancreas, pancreatic cancer and cystic fibrosis, a genetic disorder in which thick, sticky mucus can also block tubes in pancreas. Patients with type 1 diabetes may be evaluated for pancreas and kidney-pancreas transplants. Patients with type 2 diabetes are less likely to be candidates for a pancreas transplant because they may be insulin-resistant and unable to reap the benefits of a pancreas transplant.
- The pancreas is most commonly transplanted in combination with the kidney.
- There are more than 1,300 patients awaiting pancreas transplants and more than 2,100 patients awaiting combine pancreas and kidney transplants in the U.S.
_____
Intestine Transplant:
Small intestine transplants are rare and most often transplanted in combination with the liver, stomach and pancreas in small children. The intestines – both the small and large – run 25 feet long throughout our bodies, digesting food and helping the body to absorb the necessary nutrients while also getting rid of the waste products. The small intestine handles much of the nutrient absorption, while the large intestines reabsorb water from digested foods and send it back into the blood stream. The most common reason leading to transplant is short bowel syndrome caused by conditions like tumors, Crohn’s disease and other inflammatory bowel diseases, or congenital defects.
_______
Vascularized Composite Allografts:
A new form of transplantation called vascularized composite allograft (VCA) has, to date, enabled approximately 30 face transplants for people with severe facial trauma, around 70 hand transplants for amputees, a small number of uterus transplants for women without uteruses or with uterus malformations, one successful penis transplant for a man injured by an adult ritual circumcision, and another penis transplant too recent to gauge success. While not life-saving, VCAs have the potential to make life worth living for people with injuries that hinder basic human functions and prevent comfortable operation in society. In addition to being incredibly complex and expensive (health insurance will not cover VCA operation cost until proven safe and effective), these procedures have significant implications for personal identity. Unlike lungs or a kidney, faces and hands exhibit public histories of their owners, reflecting and reinforcing personality. What happens when these histories are transferred to new owners? Anecdotes from some of the first medically successful VCAs indicate a range of outcomes. Many recipients appear to be re-integrating well into their lives and careers. Some have suffered serious identity crises leading to compromised relationships, procedure reversal, and in very few instances suicide. The mental and emotional strain make standardized psychosocial screening and support a moral necessity for the field of VCA. Potential recipients and their family members should undergo extensive evaluation to ensure they are stable enough for the challenge, and long term psychotherapy should be built into the expected procedure costs.
_
Despite hands, faces, and penises having a different moral valence than solid organs, the Organ Procurement and Transplantation Network has rolled VCAs into the definition of organs for purposes of donation and transplantation. So when a person provides general consent to donation, all their parts are up for procurement. However, no online or DMV registry makes it clear that everyone has the right to opt out of VCA donation. They also do not explain that these transplants are still experimental. This information might be necessary to build an informed VCA donor pool, and to prevent some people from giving up on donating any kind of organ.
______
______
Bone marrow transplant (BMT):
Bone marrow transplantation (BMT) is now more appropriately termed hemopoietic stem cell transplantation (HSCT), as the source of the progenitor cells is no longer confined to the marrow and may be as diverse as peripheral blood and cord blood. However, the term BMT is still popularly used interchangeable with HSCT. There are similarities and differences between marrow transplant and other solid organ or tissue transplant. BMT is used mainly to treat malignant hemic disorders. Less commonly, it is used to replace defective hemopoiesis or immune systems e.g. thalassemia and aplastic anemia. Unlike solid organ transplantation, all HSCT donors are living donors and the procedure is more akin to special form of blood donation. To avoid rejection of the marrow and to minimize donor marrow attacking host tissue (graft versus host disease GVHD), HLA matching is great importance in donor choice. Usually full matching at all six A, B and DR loci are needed. Unlike blood transfusion or solid organ transplant, ABO blood group matching is not a problem. For some diseases, such as myeloma and lymphoma, the patient’s own marrow or stem cells is cryopreserved before high dose chemotherapy and is re-infused for marrow repopulation afterwards (autologous HSCT).
Umbilical cord stem cell transplant:
This may be an option if you cannot find a donor match. Cancer centers around the world use cord blood. The umbilical cord that connected a newborn to the mother during pregnancy contains blood that has been shown to contain high levels of blood stem cells. Cord blood can be collected and stored in large freezers for a long period of time and, therefore, offers another source of stem cells available for transplanting into patients.
Peripheral blood stem cells:
The same types of stem cells found in marrow can be pushed out into a donor’s bloodstream after the donor receives daily injections of a medication called filgrastim. This medication increases the number of stem cells circulating in the blood and provides a source of donor stem cells that can be collected in a way that is similar to blood donation.
Bone marrow transplant is the most widely used stem-cell therapy, but some therapies derived from umbilical cord blood are also in use. Research is underway to develop various sources for stem cells, and to apply stem-cell treatments for neurodegenerative diseases and conditions such as diabetes, heart disease, and other conditions.
_____
_____
Transplanted testicles will always make the donor’s sperm a 2018 case:
A veteran of the US Armed Forces has a new penis and scrotum after the most extensive penis transplant yet, Johns Hopkins Hospital announced recently. Not included in the transplant? Testicles — because the testicles would continue to make the donor’s sperm in the transplant recipient’s body. The patient, who asked Johns Hopkins not to reveal his name, suffered a devastating injury to his penis, testicles, part of his lower abdomen, and his legs in Afghanistan when an improvised explosive device blew. A team of 11 surgeons replaced the injured flesh of his genitals and lower abdomen with tissue from a deceased donor during a 14-hour surgery, and the patient is recovering well. But the transplant didn’t include testicles — something that the Johns Hopkins team decided early on was off the table, says Damon Cooney, a plastic and reconstructive surgery professor at the Johns Hopkins University School of Medicine. While Cooney couldn’t discuss the particulars of the situation due to confidentiality, he said that generally people who lose their testicles opt to take testosterone to replace the hormones and receive testicular prostheses to restore the appearance. Technically a testicle transplant is possible, Cooney says, and would allow recipients to forego hormone replacement therapy. But the problem is that the transplanted organ could produce the donor’s genetic offspring. And without the deceased donor’s consent, that poses an ethical complication that Johns Hopkins wanted to avoid from the outset. It’s effectively a sperm donation without consent — and that shouldn’t happen.
____
Woman to give birth after first ovary transplant pregnancy a 2018 case:
A 38-year-old woman is due to give birth after the first ever whole ovary transplant to result in a successful pregnancy. The woman, who lives in London and whose ovaries stopped working when she was 15, became pregnant just over a year after receiving a donor ovary from her identical twin sister. The transplant technique will have limited application among women who are not twins because a transplanted ovary would produce genetically different eggs. For these patients it would be simpler to have IVF with donor eggs. However, the technique offers the possibility of removing and freezing an ovary prior to cancer treatment such as radiotherapy and chemotherapy.
_____
_____
Contraindications to ODT:
The risk factors that are considered absolute contraindications for organ/tissue donation due to an increased risk of disease transmission include:
–Injection drug use, due to an increased risk of HIV, hepatitis B and C infection through sharing of putatively contaminated needles.
–Exchange of sex for money, sex with multiple partners or exposure to confirmed infected partners, given the higher odds of engaging in multiple unprotected sex acts. Epidemiological studies targeting non-intravenous drug-using patients attending clinics for sexually transmitted diseases (STD) show high prevalence of HIV, HBV and HCV among individuals with risky sexual behaviors.
–Homosexual sex among men because the literature indicates that the incidence of multiple sex partners and unprotected sex is higher among males.
Other contraindications are:
- Lack of adequate social or family support
- Significant non-compliance with medical regimen
- Central vascular disease (aortoiliac)
- Significant coronary artery disease
- Severe malnutrition/cachexia
_
President Obama’s signing of the HIV Organ Policy Equity (HOPE) Act into law 5 years ago finally made it legal for HIV-positive individuals to donate organs to HIV-positive recipients. HIV-positive individuals can now receive kidneys from HIV-positive donors, this frees up kidneys from uninfected donors for use in uninfected recipients—a win-win for everybody, as it’s illegal to transplant organs from individuals with HIV into those who don’t have the virus. There had been roughly 30 transplants from HIV-positive kidney donors to HIV-positive recipients performed in the United States.
______
______
Operative Procedure:
Organ procurement (previously called organ harvesting) is a surgical procedure that removes organs or tissues for reuse, typically for organ transplantation. It is important that the organs are retrieved in perfect condition so the organ donor’s body is treated as carefully and respectfully as if the donor were still alive. The removal of organs and tissue is no different from any other surgical operation, and is performed by highly skilled health professionals. The organs are removed and the wounds are closed using precise and sterile surgical techniques. The donation of organs and tissue does not alter the physical appearance of the body and families are encouraged to see their relative again, nor does it affect funeral arrangements.
_
If the organ donor is human, most countries require that the donor be legally dead for consideration of organ transplantation (e.g. cardiac or brain dead). For some organs, a living donor can be the source of the organ. For example, living donors can donate one kidney or part of their liver to a well-matched recipient. Organs cannot be procured after the heart has stopped beating for long time. Thus, donation after brain death is generally preferred because the organs are still receiving blood from the donor’s heart until minutes before being removed from the body and placed on ice. Donation after cardiac death (DCD) involves surgeons taking organs within minutes of the cessation of respirators and other forms of life support for patients who still have at least some brain activity. This occurs in situations where, based on the patient’s advanced directive or the family’s wishes, the patient is going to be withdrawn from life support. After this decision has been made, the family is contacted for consideration for organ donation. Once life support has been withdrawn, there is a 2-5 minute waiting period to ensure that the potential donor’s heart does not start beating again spontaneously. After this waiting period, the organ procurement surgery beings as quickly as possible to minimize time that the organs are not being perfused with blood. DCD had been the norm for organ donors until ‘brain death’ became a legal definition in the United States in 1981. Since then, most donors have been brain-dead.
_
If consent is obtained from the potential donor or the potential donor’s survivors, the next step is to perform a match between the source (donor) and the target (recipient) to reduce rejection of the organ by the recipient’s immune system. In the United States, the match between human donors and recipients is coordinated by groups like United Network for Organ Sharing. Co-ordination between teams working on different organs is often necessary in case of multiple-organ procurement. The quality of the organ then is certified. If the heart stopped beating for too long then the organ becomes unusable and cannot be used for transplant. After organ procurement the organs are often rushed to the site of the recipient for transplantation. The faster the organ is transplanted into the recipient, the better the outcome. While the organ is being transported, it is stored in an icy cold solution to help preserve it. This time during transport is called the “cold ischemia time”. Heart and lungs should have less than 6 hours between organ procurement and transplantation. For liver transplants, the cold ischemia time can be up to 10 hours, although typically surgeons aim for a much shorter period of time. For kidney transplants, as the cold ischemia time increases, the risk of delayed function of the kidney increases. Sometimes, the kidney function is delayed enough that the recipient requires temporary dialysis until the transplanted kidney begins to function.
_
Transplant surgery times differ a lot. A few examples include:
Liver, 5 to 8 hours, sometimes 12 hours
Kidney, 2 to 3 hours
Pancreas, 2 to 4 hours
Both kidney and pancreas, 5 to 7 hours
Heart transplant, 4 to 5 hours
_
Pre- and Post-transplant Monitoring:
To optimize transplantation outcomes, regular monitoring of various pre- and post-transplant factors is vital. Some of the routine monitoring tests conducted include the following:
Routine pre- and post-transplant tests: Complete blood count, chemistry screening panel, blood pressure, echocardiogram, electrocardiogram (ECG), mammogram, bronchoscopy, pulmonary function test (PFT), ultrasonography and biopsies
Pre- and post-transplant serological screening for infectious diseases: Human immunodeficiency virus (HIV), hepatitis A, B, and C viruses, cytomegalovirus (CMV), herpes simplex virus, Epstein-Barr virus (EBV), toxoplasmosis, and varicella-zoster virus and measles virus (in pediatric patients)
Monitoring for organ function: Tests for monitoring toxic side effects of immunosuppressive drugs and the graft function for some of the organs include:
- Kidney: cystatin C, urinary proteins, creatinine, and blood urea nitrogen (BUN)
- Heart: troponin I, creatine kinase muscle-brain fraction isoenzyme (CK-MB), high sensitivity C-reactive protein (hsCRP), lipid profile, and apolipoproteins
- Liver: liver enzymes, albumin, protein C, and prothrombin time (PT)
- Pancreas: glycosylated hemoglobin (HbA1c), glucose, lipase, amylase, and urinalysis
Early detection of acute phase reactions and complications: hsCRP, serum amyloid A protein (SAA), and cystatin C are monitored.
Assays of coagulation factors:
The quantitative assay of coagulation parameters is determined by standard coagulation tests, such as PT, PTT, and platelet count. These parameters do not help in the qualitative assessment of the clot formation and hence are non-reliable. For e.g., the diagnosis of fibrinolysis, a major cause of persistent coagulopathy unresponsive to conventional treatment in liver transplant patients, cannot be made by the usual coagulation tests, mandating the need for a Thromboelastogram (TEG). Transplantation of the heart, heart and lungs, and liver, in particular, place a significant burden on the patient’s coagulation system. Cardiopulmonary bypass for heart transplant requires systemic anticoagulation and results in bypass-related platelet and coagulation dysfunction.
_____
Transfusion Support in Solid-Organ Transplantation:
The typical requirements for blood components for each type of organ transplant in adults are shown below.
| Median Blood Use (Units) in Organ Transplantation | |||
| Organ | Red cells | Plasma | Platelets |
| Liver | 12 | 13 | 10 |
| Heart | 4 | 5 | 10 |
| Lung | |||
| Single | 0-2 | – | – |
| Double | 7 | 2 | 8 |
| Kidney | 0-2 | – | – |
Liver transplant procedures require the most blood components despite the fact that blood use in liver transplantation has declined dramatically over the last decade. The multiple factors contributing to the reduction in blood usage include: improved surgical technique, organ preservation, and anaesthetic management, as well as better intraoperative monitoring of coagulation status and pharmacologic treatment of fibrinolysis. Heart transplantation is associated with lower blood requirements that approximate blood usage observed in complex cardiopulmonary bypass procedures. Blood usage in lung transplantation varies by the type of lung transplant procedure. More than 2/3 of single-lung transplant recipients do not require any transfusions. Double-lung transplant procedures typically require more red cells than heart transplant procedures. The majority of patients receiving kidney transplants do not require blood. For solid-organ transplant procedures other than liver, transfusion requirements are generally not sufficient to require deviation from traditional selection criteria of ABO identical/compatible red cells. However, in liver transplantation, transfusions frequently exceed the available supply of ABO identical red cells, antigen-negative red cells, or compatible plasma, and thus require blood bank blood group switching protocols to optimally use available blood resources.
_
Role of transfusion in transplant:
Blood products are used either for improving hemoglobin levels or facilitating coagulation or sometimes for both. In addition, blood transfusion is also used specifically for its immune-modifying effect which can favorably alter the transplant outcome. Opelz et al found out that blood transfusion enhanced renal graft survival. They subsequently demonstrated that this response was transfusion dose-dependent and white cell-depleted red cells were less effective in promoting graft survival. Transfusion-associated immunosuppression has been well documented and favorably utilized in other conditions, such as in women with recurrent abortions who shared a HLA type with their husbands. Similar suppression of cytotoxic T-lymphocytes may play a role in graft survival. With the rapid improvement in immunosuppression therapy, the additional effect of transfusion became marginal. The relevance of such protocols in clinical practice has diminished due to the improvement in HLA technology and remarkable advances in targeted and safe immunosuppression. More recent experience suggests no difference in graft survival between transfused and non-transfused organ recipients.
_______
What Precautions do I need to take after an Organ Transplant?
Right after an organ transplant, you’re particularly vulnerable. You’ll be in the induction phase of immunosuppression. You’ll be on pretty high doses; it’s key that you take extra care. You should:
- Wash your hands often. Hand washing is an excellent way to reduce exposure to germs. It’s especially important before you eat.
- Avoid people who are sick. It’s best to limit contact with anyone who has a cold or any other infection like measles or chicken pox.
- Avoid people who have been recently vaccinated. Some vaccines, such as the new nasal flu vaccine or the measles vaccine, have a living virus in them. These could be a risk to people with weak immune systems.
- Stay out of crowded areas. For example, avoid malls and movie theatres.
- Don’t take care of pets. Pets carry germs, so limit your exposure to them. You don’t have to kick them out of the house. Instead, look at this as an excuse to make your spouse or kids clean out the litter box for a change.
- Don’t garden. Some dangerous bacteria live in the soil. So let your garden go wild for a few months. Or hire someone to do the weeding for you.
- Brush and floss daily. Both help keep your mouth free of infections. Have your teeth cleaned regularly.
- Don’t ignore cuts or scratches. Clean them and put on a bandage. Get in touch with your health care provider if you have any signs of infection.
- Practice safe sex. Sexually transmitted diseases such as herpes can be a problem for anyone. But they can be dangerous for people who have had an organ transplant. Condoms may not be enough to fully protect you. Even saliva can expose you to colds and viruses. So be careful. Ask your health care provider about what’s safe in your case.
Obviously, specific recommendations depend on your health and situation. Where you live can even make a difference. If you’re in a city, it’s harder to avoid crowds. Living in the country poses different risks, such as exposure to farm animals or potentially unsafe well water. Ask your health care adviser for recommendations.
_
Lifetime Precautions after an Organ Transplant:
Over the next six months to a year after an organ transplant, your health care team will probably reduce your medication. You’ll settle into the “maintenance phase” on a lower dose. At this point, you can usually relax some of your safety measures. You won’t be as susceptible to infection. But you should still take precautions. Wash your hands regularly and limit contact with people who are sick or recently vaccinated. If you ever have an episode where your body rejects a donor organ (organ rejection), your doctor may need to change your medications or boost the dosage of immunosuppressant drugs. This is called “anti-rejection immunotherapy.” Since your immune system will be further suppressed, you’ll need to take those extra precautions again. Your doctor may also occasionally need to change some of the medicines. Some may not work as well over time. New and more effective drugs may also come on the market that will replace old ones.
______
_____
ODT outcome and graft survival:
_
Not necessarily a cure:
While an organ transplant can transform or lengthen the life of a person who is dying, it’s important to know that survival rates differ for each individual and procedure. Several factors of aftercare, such as diet, lifestyle and medication also play a big role in the outcome of the surgery and the survival of the patient. The lifespan and survival rate of transplanted organs depend on several factors, including the patient’s aftercare, the possibility of chronic rejection, how effectively the organ was cooled, and how long it took for the organ to reach the recipient. Most medical experts agree that organ transplants are not necessarily a cure for a disease – it is basically swapping one chronic condition for another, since the patient will have to be on lifelong immunosuppressant medication to combat rejection.
_
Although HLA matching significantly improves the success rate of clinical organ transplantation, it does not in itself prevent rejection reactions. There are two main reasons for this. First, HLA typing is imprecise, owing to the polymorphism and complexity of the human MHC; unrelated individuals who type as HLA-identical with antibodies against MHC proteins rarely have identical MHC genotypes. This should not be a problem with HLA-identical siblings: because siblings inherit their MHC genes as a haplotype, one sibling in four should be truly HLA-identical. Nevertheless, grafts between HLA-identical siblings are invariably rejected, albeit more slowly, unless donor and recipient are identical twins. This rejection is the result of differences between minor histocompatibility antigens, which is the second reason for the failure of HLA matching to prevent rejection reactions. Thus, unless donor and recipient are identical twins, all graft recipients must be given immunosuppressive drugs to prevent rejection. Indeed, the current success of clinical transplantation of solid organs is more the result of advances in immunosuppressive therapy than of improved tissue matching. The limited supply of cadaveric organs, coupled with the urgency of identifying a recipient once a donor organ becomes available, means that accurate matching of tissue types is achieved only rarely.
_
In MHC-identical grafts, rejection is caused by peptides from other alloantigens bound to graft MHC molecules:
When donor and recipient are identical at the MHC but differ at other genetic loci, graft rejection is not so rapid. The polymorphic antigens responsible for the rejection of MHC-identical grafts are therefore termed minor histocompatibility antigens or minor H antigens. Responses to single minor H antigens are much less potent than responses to MHC differences because the frequency of responding T cells is much lower. However, most inbred mouse strains that are identical at the MHC differ at multiple minor H antigen loci, so grafts between them are still uniformly and relatively rapidly rejected. The cells that respond to minor H antigens are generally CD8 T cells, implying that most minor H antigens are complexes of donor peptides and MHC class I molecules. However, peptides bound to MHC class II molecules can also participate in the response to MHC-identical grafts.
_
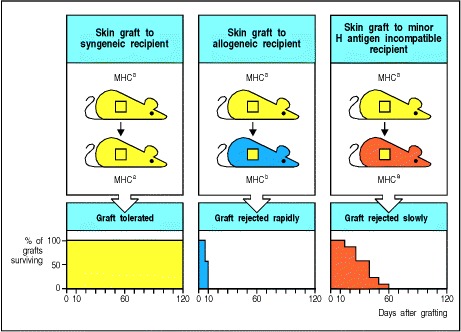
Figure above shows that even complete matching at the MHC does not ensure graft survival. Although syngeneic grafts are not rejected (left panels), MHC-identical grafts from donors that differ at other loci (minor H antigen loci) are rejected (right panels), albeit more slowly than MHC-disparate grafts (center panels).
_
What other factors increase chance for a successful organ transplant?
Other things that affect your chance of having a successful organ transplant include:
- The age of the donor organ. In general, the younger the organ donor, the healthier the tissue. But recent research is challenging this thought. It may be that some older organs work just as well as younger organs.
- The length of time that the donor organ is out of the donor’s body. The more quickly an organ is transplanted after it is removed from the donor, the more viable the organ tissue remains. Transplant team will make every effort to quickly transfer the donor organ.
- How well the organ was preserved just before transplantation. The donor organ must be properly preserved while it is being transferred, especially if it was transferred from a long distance. Transplant team will make every effort to make sure the donor organ is properly transferred to your location.
_
Traditionally, graft acceptance has depended on a large number of variables including the overall health of the donor and recipient, the state of the organ or tissue at the time of recovery, and the time between death and recovery which affect the degree of oxidative damage and ischemia, the technical success of the transplantation procedure itself and the degree of immunocompatibility between the donor and the recipient. Much focus has been placed on the means to prevent immune rejection of the graft. Immunosuppressive agents have been quite successful, however, the level of associated toxicity of the currently prescribed agents and their potentially life-threatening side-effects that result after years of administration necessitates new, specific therapies.
_
The survival rate of an organ transplant is distinguished between patient survival (calculated from the date of the transplant to the date of the patient’s death) and graft survival (an estimated probability of the survival of the organ from the date of the transplant until the first signs of failure).
_
Outcomes of organ transplantation:
The benefit of transplantation is to be evaluated in the long term. As an example, the following illustration brings together data on the percentage of survival for transplanted kidneys after one year from various countries and teams around the world. These data are available on the web site of national transplantation organizations or have been published in medical and scientific literature. They are a demonstration that kidney transplantation yields good outcomes in all contexts. It also shows that the difference in results between transplanted kidneys from living and from deceased donors is small, a fact that encourages the use of organs donated from cadavers whenever possible rather than taking the risk, however small, of harming a living donor.
![]()
Scientific and professional societies have an essential role in monitoring the outcomes of transplantation and of living donations.
_
Transplanted organs don’t last forever:
While transplanting a healthy organ to replace a diseased or failed organ can prolong life, transplants have limits. A kidney transplant does not last for ever. The average life-span of a transplanted kidney is twelve years for a deceased donor kidney, and about 15 years for a living related transplant. The average for a living unrelated transplant is somewhere between the two. So, the ‘best’ (longest lasting) kidney transplant is one from a relative, then a friend or partner, then a dead person. A transplanted pancreas keeps working for five years in only 57 percent of patients, meaning nearly half of patients will need a second transplant. A transplanted liver will function for five years or more in 70 percent of recipients, and even longer if the organ came from a living donor. After a heart transplant, the five-year survival rate for the organ is about 76 percent. However, a transplanted lung continues to work for five years or more in only about 52 percent of patients, according to the Scientific Registry of Transplant Recipients.
_
Transplant stats:
The odds for long-term transplant success remain stubbornly low, as shown for some of the most-transplanted organs.
55% Proportion of kidneys transplanted in the U.S. in 2006 that survived at least 10 years
56% Proportion of livers transplanted in the U.S. in 2006 that survived at least 10 years
58% Proportion of hearts transplanted in the U.S. in 2006 that survived at least 10 years
30% Proportion of lungs transplanted in the U.S. in 2006 that survived at least 10 years
_
Procedures to enhance graft survival:
In clinical practice, the most successful transplantation programs have been with kidneys and corneas. However, other organs are being transplanted with increasing frequency. The success in these programs has been due to a better understanding of immunological mechanisms, definition of MHC antigens and development of more effective immunosuppressive agents.
- Donor selection
Based on extensive experiences with renal transplants, certain guidelines can be followed in donor selection and recipient preparation for most organ transplants. The most important in donor selection is the MHC identity with the recipient; an identical twin is the ideal donor. Grafts from an HLA-matched sibling have 95-100% chance of success. One haplotype-identical parent or sibling must match at the HLA D region. A two haplotype-distinct donor with a reasonable match for D-region antigen can also be used. Organs from a two or one DR matched cadaver have been used also with some success. In every case, an ABO compatibility is essential.
- Recipient preparation
The recipient must be infection-free and must not be hypertensive. One to five transfusions of 100-200 ml whole blood from the donor at 1-2 week intervals improves the graft survival and is practiced when possible.
- Immunosuppression
Immunosuppressive therapy is most essential part of allo-transplantation. The most recent and effective family of agents is cyclosporin A, FK-506 (tacrolimus) and rapamycin. Cyclosporin A and FK506 inhibit IL-2 synthesis following Ag-receptor binding whereas rapamycin interferes with signal transduction following IL2 – IL2 receptor interaction. Thus, all three agents block T cell proliferation in response to antigen. Immunosuppression is discussed later on. Whole body irradiation is used in leukemia patients before bone marrow transplantation. Antisera against T cells (anti-thymocyte globulin: ATG) or their surface antigens (CD3, CD4, CD45 on activated T-cells, CD25:IL-2 receptors) are being used also to achieve immunosuppression.
______
______
Signs of organ transplant rejection:
After a transplant, such as a kidney transplant, specific drugs have to be taken for life to help prevent the body rejecting the new organ. Transplant patients need to watch out for signs of organ rejection. These include:
- Pain at the site of the transplant
- Feeling unwell
- Irritability (in children)
- Flu-like symptoms
- Fever
- Weight changes
- Swelling
- Change in heart rate
- Passing urine less often
Seek medical advice straight away if you have any of these symptoms.
_
Clinical Stages of Rejection:
- Hyperacute rejection:
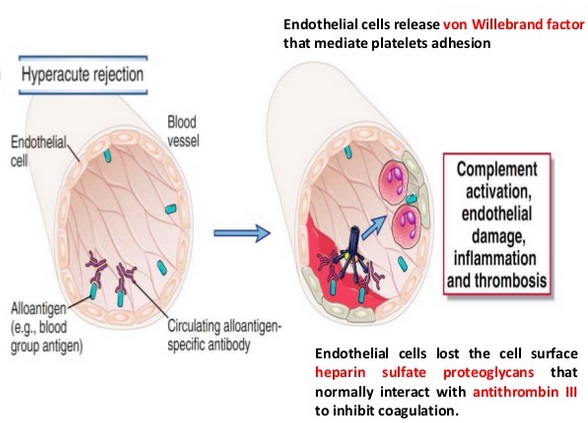
Figure above shows antibodies reacting with endothelium cause hyperacute graft rejection.
Hyperacute rejection appears in the first minutes following transplantation and occurs only in vascularized grafts. In hyperacute rejection, the transplanted tissue is rejected within minutes to hours because vascularization is rapidly destroyed. Antibody responses are also an important potential cause of graft rejection. Preexisting alloantibodies to blood group antigens and polymorphic MHC antigens can cause rapid rejection of transplanted organs in a complement-dependent reaction that can occur within minutes of transplantation. This type of reaction is known as hyperacute graft rejection. Most grafts that are transplanted routinely in clinical medicine are vascularized organ grafts linked directly to the recipient’s circulation. In some cases, the recipient might already have circulating antibodies against donor graft antigens, produced in response to a previous transplant, pregnancy or a blood transfusion. Such antibodies can cause very rapid rejection of vascularized grafts because they react with antigens on the vascular endothelial cells of the graft and initiate the complement and blood clotting cascades. The vessels of the graft become blocked, causing its immediate death. Such grafts become engorged and purple-colored from hemorrhaged blood, which becomes deoxygenated. The kidney is most susceptible to hyperacute rejection; the liver is relatively resistant, possibly because of its dual blood supply, but more likely because of incompletely understood immunologic properties. Today, this type of rejection is avoided in most cases by checking for ABO compatibility and by excluding the presence of antidonor human leukocyte antigen (HLA) antibodies by cross-match techniques between donor graft lymphocytes and recipient sera. This type of rejection is also observed in models of xenotransplantation of vascularized organs between phylogenetically distant species when no immunosuppressive treatment is given to the recipients. This is an irreversible event, and the only treatment option is immediate graft removal.
_
Accelerated rejection occurs on the third to the fifth day after kidney transplantation. It is accompanied by fever, graft swelling, oliguria, and tenderness. It is thought to be mediated by non–complement-fixing antibodies to antigens present in the donor kidney. Histopathologically, it is characterized by vascular disruption with hemorrhage. The most effective treatments are anti-lymphocyte reagents, with or without plasmapheresis; these have a success rate of about 60% in reversing this process.
_
- Acute rejection:
Acute rejection manifests commonly in the first 6 months after transplantation.
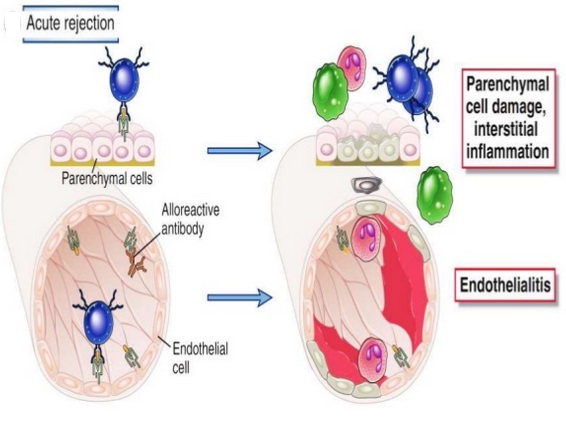
Acute cellular rejection is mediated by lymphocytes that have been activated against donor antigens, primarily in the lymphoid tissues of the recipient. The donor dendritic cells (also called passenger leukocytes) enter the circulation and function as antigen-presenting cells (APCs). Acute rejection is caused by an immune response directed against the graft and occurs between 1 week and several months after transplantation. Acute rejection is diagnosed on histological analysis of a graft biopsy according to an international classification system, the Banff classification for the kidney (Mengel et al. 2012). Acute rejection is thought to result from two immunological mechanisms that may act alone or in combination: (1) a T-cell-dependent process that corresponds to acute cellular rejection, and (2) a B-cell-dependent process that generates the acute humoral rejection. With current immunosuppressive treatment, acute rejection occurs in less than 15% of the transplants (Port et al. 2004) in nonsensitized patients. High-dose pulses of steroids and antilymphocyte reagents are effective in reversing the T-cell response about 80% to 90% of the time, but antilymphocyte antibodies only reverse the vasculitis about 60% of the time.
_
Frequency of acute reaction:
Following transplantation, the transplanted organ is at risk for rejection. The frequency of acute rejection episodes varies depending on which organ is transplanted. The highest incidence of acute rejection is shown after lung, heart, and intestinal transplantation (~35%–40%, 30%–45%, and 55%, respectively). Liver and kidney transplantation generally shows less frequent episodes of acute rejection, with incidences of 13%–30% and 12%–14%, respectively. The surveillance of organ functionality, particularly to detect the onset of rejection, is a crucial task for the long-term viability of the graft. Usually, diagnosis of acute rejection relies on clinical signs, but laboratory data such as blood markers (lipase/amylase in pancreas transplantation, creatinine in kidney transplantation, and liver enzymes in liver transplantation) are invaluable tools to monitor graft function.
_
- Chronic rejection:
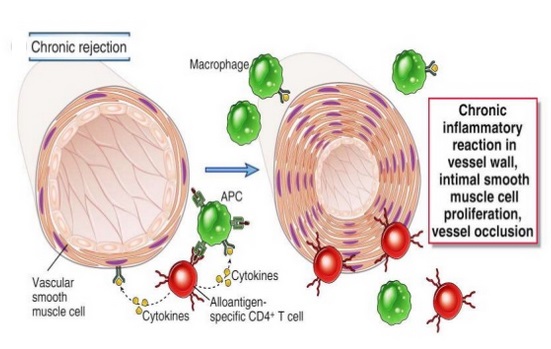
Chronic rejection is now the leading cause of graft rejection. Chronic rejection can be mediated by either humoral or cellular mechanisms linked to memory/plasma cells and antibodies. The presence of tertiary lymphoid organs in the graft is a characteristic of this form of rejection. Chronic rejection develops months to years after acute rejection episodes have subsided. The use of immunosuppressive drugs and tissue-typing methods has increased the survival of allografts in the first year, but chronic rejection is not prevented in most cases. Chronic rejection appears as fibrosis and scarring in all transplanted organs, but the specific histopathological picture depends on the organ transplanted. In heart transplants, chronic rejection manifests as accelerated coronary artery atherosclerosis. In transplanted lungs, it manifests as bronchiolitis obliterans. In liver transplants, chronic rejection is characterized by the vanishing bile duct syndrome. In kidney recipients, chronic rejection (called chronic allograft nephropathy) manifests as fibrosis and glomerulopathy. This process is usually treatment-resistant, although progression may be slowed by immunosuppressive regimens.
The following factors increase the risk of chronic rejection:
- Previous episode of acute rejection
- Inadequate immunosuppression
- Initial delayed graft function
- Donor-related factors (e.g., old age, hypertension)
- Reperfusion injury to organ
- Long cold ischemia time
- Recipient-related factors (e.g., diabetes, hypertension, hyperlipidemia)
- Posttransplant infection (e.g., cytomegalovirus [CMV])
_
Chronic rejection can be broadly defined as a largely indolent, but progressive form of allograft injury characterized primarily by fibrointimal hyperplasia of arteries, or obliterative arteriopathy (OA), interstitial fibrosis and atrophy of parenchymal elements. For the most part, it is irreversible and eventually results in allograft failure. Currently, chronic rejection is the most significant medical obstacle to long term morbidity-free allograft survival. The incidence is thought to progressively increase with time after transplantation, but after a period of five years it affects about 10% of liver to around 60% of lung allograft recipients (table below).
Estimates of the incidence of chronic rejection (CR) in various solid organ allografts:
| Allograft | Incidence of OA at 5 Years |
| Heart | 25% – 60% |
| Heart-Lung | 8% – 20% (obliterative arteriopathy) |
| 50% – 60% (obliterative bronchiolitis) | |
| Lung | 28/45% (single/double lung) |
| Liver | 3–17%; 10% and decreasing |
| Pancreas alone | 30–70%*(late graft loss) |
| Pancreas and kidney | 20–40%* |
*Estimates based on graft survival rates after one year, with the assumption that most late graft failures are due to CR. At least 50% of the patients with renal transplant develop features of chronic allograft nephropathy (CAN) within 10 years of their transplant.
_____
_____
Molecular assessment of disease states in kidney transplant biopsy samples a 2016 study:
Progress in renal transplantation requires improved understanding and assessment of rejection and injury. Study of the relationship between gene expression and clinical phenotypes in kidney transplant biopsy samples has led to the development of a system that enables diagnoses of specific disease states on the basis of messenger RNA levels in the biopsy sample. Using this system authors have defined the molecular landscape of T cell-mediated rejection (TCMR), antibody-mediated rejection (AMR), acute kidney injury (AKI), and tubular atrophy and interstitial fibrosis. TCMR and AMR share IFNγ-mediated effects and TCMR has emerged as a cognate T cell antigen presenting cell process in the interstitium, whereas AMR is a natural-killer-cell-mediated process that occurs in the microcirculation. The specific features of these different processes have led to the creation of classifiers to test for TCMR and AMR, and revealed that AMR is the principal cause of kidney transplant deterioration. The molecular changes associated with renal injury are often more extensive than suggested by histology and indicate that the progression to graft failure is caused by continuing nephron injury, rather than fibrogenesis. In summary, advances in the molecular assessment of disease states in biopsy samples has improved understanding of specific processes involved in kidney graft outcomes.
____
The importance of non-HLA antibodies in transplantation a 2016 study:
The development of post-transplantation antibodies against non-HLA autoantigens is associated with rejection and decreased long-term graft survival. Although our knowledge of non-HLA antibodies is incomplete, compelling experimental and clinical findings demonstrate that antibodies directed against autoantigens such as angiotensin type 1 receptor, perlecan and collagen, contribute to the process of antibody-mediated acute and chronic rejection. The mechanism that underlie the production of autoantibodies in the setting of organ transplantation is an important area of ongoing investigation. Ischaemia reperfusion injury, surgical trauma and/or alloimmune responses can result in the release of organ-derived autoantigens (such as soluble antigens, extracellular vesicles or apoptotic bodies) that are presented to B cells in the context of the transplant recipient’s antigen presenting cells and stimulate autoantibody production. Type 17 T helper cells orchestrate autoantibody production by supporting the proliferation and maturation of autoreactive B cells within ectopic tertiary lymphoid tissue. Conversely, autoantibody-mediated graft damage can trigger alloimmunity and the development of donor-specific HLA antibodies that can act in synergy to promote allograft rejection. Identification of the immunologic phenotypes of transplant recipients at risk of non-HLA antibody-mediated rejection, and the development of targeted therapies to treat such rejection, are sorely needed to improve both graft and patient survival.
_______
_______
The converse of transplant rejection is graft-versus-host disease (GVHD):
Allogeneic bone marrow transplantation is a successful therapy for some tumors derived from bone marrow precursors, such as certain leukemias and lymphomas. It may also be successful in the treatment of some primary immunodeficiency diseases and inherited bone marrow diseases, such as the severe forms of thalassemia. In leukemia therapy, the recipient’s bone marrow, the source of the leukemia, must first be destroyed by aggressive cytotoxic chemotherapy. One of the major complications of allogeneic bone marrow transplantation is graft-versus-host disease (GVHD), in which mature donor T cells that contaminate the allogeneic bone marrow recognize the tissues of the recipient as foreign, causing a severe inflammatory disease characterized by rashes, diarrhea, and pneumonitis. Graft-versus-host disease occurs not only when there is a mismatch of a major MHC class I or class II antigen but also in the context of disparities between minor H antigens. Graft-versus-host disease is a common complication in recipients of bone marrow transplants from HLA-identical siblings, who typically differ from each other in many polymorphic proteins encoded by genes unlinked to the MHC.
_
The presence of alloreactive T cells can easily be demonstrated experimentally by the mixed lymphocyte reaction (MLR), in which lymphocytes from a potential donor are mixed with irradiated lymphocytes from the potential recipient. If the donor lymphocytes contain alloreactive T cells, these will respond by cell division. The MLR is sometimes used in the selection of donors for bone marrow transplants, when the lowest possible alloreactive response is essential. However, the limitation of the MLR in selection of bone marrow donors is that the test does not accurately quantitate alloreactive T cells. A more accurate test is a version of the limiting-dilution assay, which precisely counts the frequency of alloreactive T cells.
_
Although graft-versus-host disease is usually harmful to the recipient of a bone marrow transplant, there can be some beneficial effects. Some of the therapeutic effect of bone marrow transplantation for leukemia can be due to a graft-versus-leukemia effect, in which the allogeneic bone marrow recognizes minor H antigens or tumor-specific antigens expressed by the leukemic cells, leading the donor cells to kill the leukemic cells. One such minor H antigen, HB-1, is a B-cell lineage marker that is expressed by acute lymphoblastic leukemia cells, which are B-lineage cells, and by B lymphocytes transformed with Epstein-Barr virus (EBV). One of the treatment options for suppressing the development of graft-versus-host disease is the elimination of mature T cells from the donor bone marrow in vitro before transplantation, thereby removing alloreactive T cells. Those T cells that subsequently mature from the donor marrow in vivo in the recipient are tolerant to the recipient’s antigens. Although the elimination of graft-versus-host disease has benefits for the patient, there is an increase in the risk of leukemic relapse, which provides strong evidence in support of the graft-versus-leukemia effect.
_
GVHD pathology:
Billingham Criteria:
Three criteria must be met in order for GVHD to occur.
- An immuno-competent graft is administered, with viable and functional immune cells.
- The recipient is immunologically different from the donor – histo-incompatible.
- The recipient is immuno-compromised and therefore cannot destroy or inactivate the transplanted cells.
The pathophysiology of GVHD includes three phases:
- Activation of APC (antigen presenting cells)
- Activation, proliferation, differentiation and migration of effector cells
- Target tissue destruction
Activation of APC occurs in the first stage of GVHD. Prior to haematopoietic stem cell transplantation, radiation or chemotherapy results in damage and activation of host tissues, especially intestinal mucosa. This allows the microbial products to enter and stimulate pro-inflammatory cytokines such as IL-1 and TNF-α. These proinflammatory cytokines increase the expression of MHC and adhesion molecules on APCs, thereby increasing the ability of APC to present antigen. The second phase is characterized by the activation of effector cells. Activation of donor T-cells further enhances the expression of MHC and adhesion molecules, chemokines and the expansion of CD8 + and CD4 + T-cells and guest B-cells. In the final phase, these effector cells migrate to target organs and mediate tissue damage, resulting in multiorgan failure.
_
Prevention:
- DNA-based tissue typing allows for more precise HLA matching between donors and transplant patients, which has been proven to reduce the incidence and severity of GVHD and to increase long-term survival.
- The T-cells of umbilical cord blood (UCB) have an inherent immunological immaturity, and the use of UCB stem cells in unrelated donor transplants has a reduced incidence and severity of GVHD. The use of liver-derived hematopoietic stem cells to reconstitute bone marrow has the highest success rate according to recent studies.
- Methotrexate, cyclosporine and tacrolimus are common drugs used for GVHD prophylaxis.
- Graft-versus-host-disease can largely be avoided by performing a T-cell-depleted bone marrow transplant. However, these types of transplants come at a cost of diminished graft-versus-tumor effect, greater risk of engraftment failure, or cancer relapse, and general immunodeficiency, resulting in a patient more susceptible to viral, bacterial, and fungal infection. In a multi-center study, disease-free survival at 3 years was not different between T cell-depleted and T cell-replete transplants.
Treatment:
Intravenously administered glucocorticoids, such as prednisone, are the standard of care in acute GVHD and chronic GVHD. The use of these glucocorticoids is designed to suppress the T-cell-mediated immune onslaught on the host tissues; however, in high doses, this immune-suppression raises the risk of infections and cancer relapse. Therefore, it is desirable to taper off the post-transplant high-level steroid doses to lower levels, at which point the appearance of mild GVHD may be welcome, especially in HLA mis-matched patients, as it is typically associated with a graft-versus-tumor effect. Cyclosporine and tacrolimus are inhibitors of calcineurin. Both substances are structurally different but have the same mechanism of action. Cyclosporine binds to the cytosolic protein Peptidyl-prolyl cis-trans isomerase A (known as cyclophilin), while tacrolimus binds to the cytosolic protein Peptidyl-prolyl cis-trans isomerase FKBP12. These complexes inhibit calcineurin, block dephosphorylation of the transcription factor NFAT of activated T-cells and its translocation into the nucleus. Standard prophylaxis involves the use of cyclosporine for six months with methotrexate. Cyclosporine levels should be maintained above 200 ng/ml. Other substances that have been studied for GVHD prophylaxis include, for example: sirolimus, pentostatin and alemtuzamab. In August 2017 the US FDA approved ibrutinib to treat chronic GVHD after failure of one or more other systemic treatments.
_____
Graft-versus-tumor effect:
Graft-versus-tumor effect (GvT) appears after allogeneic hematopoietic stem cell transplantation (HSCT). The graft contains donor T cells (T lymphocytes) that can be beneficial for the recipient by eliminating residual malignant cells. GvT might develop after recognizing tumor-specific or recipient-specific alloantigens. It could lead to remission or immune control of hematologic malignancies. This effect applies in myeloma and lymphoid leukemias, lymphoma, multiple myeloma and possibly breast cancer. It is closely linked with graft-versus-host disease (GVHD), as the underlying principle of alloimmunity is the same. CD4+CD25+ regulatory T cells (Treg) can be used to suppress GVHD without loss of beneficial GvT effect. The biology of GvT response still isn’t fully understood but it is probable that the reaction with polymorphic minor histocompatibility antigens expressed either specifically on hematopoietic cells or more widely on a number of tissue cells or tumor-associated antigens is involved. This response is mediated largely by cytotoxic T lymphocytes (CTL) but it can be employed by natural killers (NK cells) as separate effectors, particularly in T-cell-depleted HLA-haploidentical HSCT.
_____
_____
Non-immune Mechanisms of Graft Failure:
There are many reasons why a kidney transplant can fail besides immune mediated rejection:
- Clot: This is usually when the blood vessels to the transplanted kidney clot, so the kidney has no blood flow. This seems most likely to happen shortly after the surgery.
- Fluid collection: If there is fluid collection around the kidney, there can be damage to the kidney from the pressure if it is not treated.
- Infection: Having an infection in the kidney can cause permanent problems with the kidney, especially if it is not found and treated early.
- Side effect of medicines: Some medicines can be harmful to kidneys.
- Donor kidney problems: Transplant surgeons will only offer you a kidney that they believe will work, but sometimes there are problems with the donor kidney that are not expected and the kidney never works well. If the kidney never works well, it is not likely to last long.
- Recurrent Disease: Although it is not very common, it is possible for the disease that damaged your original kidneys to come back and damage the transplanted kidney. Some of the processes that led to the failure of the patient’s own liver can damage the new liver and eventually destroy it. Perhaps the best example is hepatitis B infection. In the early 1990’s, patients who received liver transplants for hepatitis B infection had less than 50% five year survival. The vast majority of these patients suffered from very aggressive reinfection of the new liver by hepatitis B virus. During the 1990’s, however, several drugs and strategies to prevent re-infection and damage of the new liver were developed and instituted widely by transplant centers. These approaches have been highly successful such that recurrent disease is no longer a problem. Hepatitis B, once considered a contra-indication to transplantation, is now associated with excellent outcomes, superior to many of the other indications for liver transplantation. Currently, our primary problem with recurrent disease is focused on hepatitis C. Any patient that enters transplantation with hepatitis C virus circulating in their blood will have ongoing hepatitis C after transplantation. However, those who have completely cleared their virus and do not have measurable hepatitis C in the blood will not have hepatitis C after transplantation.
Several other diseases may also recur after transplantation, but typically the disease is mild and only slowly progressive. Primary sclerosing cholangitis (PSC) and primary biliary cirrhosis (PBC) both recur approximately 10-20% of the time and, only very rarely, result in recurrent cirrhosis and end stage liver disease. Perhaps the biggest unknown in today’s age is fatty liver disease after transplantation as it is clearly a problem of increasing frequency. Fatty liver disease can occur in those transplanted for NASH but also in patients who were transplanted for other indications and develop risk factors for fatty liver disease. The frequency, trajectory, and prognosis of recurrence of fatty liver disease after transplant and its course are active areas of research.
______
______
Transplant biomarkers:
To be sure, organ transplants save lives. More than 33,000 organs were transplanted in the U.S. in 2016, the most recent year for which data are available, according to the United Network for Organ Sharing. In the real world, though, after a transplant, a recipient’s immune system fights against the organ, recognizing it as foreign. As many as 15% of people receiving kidney transplants, for instance, experience acute rejection, meaning that the immune system sends in its troops and causes inflammation within the first year. For those patients, the story line isn’t tied up neatly. Rejection episodes like these are usually treatable and reversible. So “rejection” doesn’t necessarily mean the transplanted organ—or graft, as doctors like to call it—is lost. Tissue damage can occur during these episodes, however, and if it happens enough times or is not treated quickly enough, the organ fails.
_
Transplantation rejection monitoring aims to increase the survival rate of transferred organs through forecasting and diagnosing any emergency situations which can be derived by any immunological rejections after an organ transfer and by minimizing the use of immuno-suppressor. Until now, only invasive method biopsy of transplanted organs was examined which is costly and accompanies various side effects. Researchers are currently developing a non-invasive method for monitoring rejection of organ transplants. To ensure prompt treatment, physicians need a way to monitor organ function and diagnose rejection. The only method available to them now is direct biopsy of the transplant. In the case of a kidney transplant, the typical schedule for routine monitoring is to take biopsies of the organ at one week, one month, three months, six months, one year, and yearly after that. Rather than poke a needle into an organ to sample cells and tissues—a risky venture—doctors would prefer to noninvasively measure molecular markers in a person’s blood and urine to monitor recovery. These markers, typically nucleic acids and proteins, could help indicate when a transplanted organ has started to fail, help guide treatments, minimize the number of biopsies needed, and ultimately improve transplant success rates.
_
Biomarkers that indicate how a person’s immune system is functioning could help guide doctors in prescribing the correct dose of immunosuppressants for individual transplant patients to help ward off acute rejection. And they might someday help develop a treatment for chronic rejection. Most transplants are treated the same. At most centers, patients receive therapy to dial down the immune system at the time of the transplant. After the transplant, they receive multiple immunosuppressant drugs. Because doctors don’t have a tool to measure immune function, they usually give all patients the same amount of medication. Physicians typically wait six months and slowly lower the dose of one of the drugs. They don’t really measure anything. They just wait and see what happens. Such an approach means that some people receive more drug than they need, whereas others receive less. Both of these options can have negative consequences. Too much drug suppresses the immune system too much, leaving a patient susceptible to infections. Side effects of overprescribing immunosuppressants are a major factor in the premature death of transplant recipients. At the other extreme, too little drug can pave the way for rejection and organ loss. Physicians want to avoid both of these situations and tailor the amount of immunosuppressants that patients receive. But the only way that physicians currently have for determining whether they should adjust a patient’s drug dose is to take a biopsy. There are complications that come from putting a needle into an organ with lots of vessels. Beyond the risk of bleeding, there’s the time, expense, and patient anxiety to contend with. Biomarkers that signal rejection could offer such a diagnostic to avoid invasive biopsy. With the advancement of technology, biomarkers will be developed that not only tell us the diagnosis but also the severity of the disease.
_
Biomarkers need to go through many stages before they can be used in clinical practice. In the case of transplant rejection, candidate biomarkers are still waiting for prospective clinical trials. After those trials, the biomarkers will still need to go through commercialization and final implementation. None of the transplant biomarkers have yet reached that stage. Current biomarkers fall short of that goal. For example, in the case of kidney function, physicians for decades have been limited to creatinine as a biomarker. Inside the body, the level of creatinine—a breakdown product of muscle—remains fairly constant. It’s the kidneys’ job to filter the chemical from the body, so changes in the amount of creatinine in urine can signal problems with the organs’ function. But creatinine is an inaccurate biomarker. Yes, it can be detected noninvasively in a patient’s serum without doing a biopsy. But its levels increase only after major damage to the kidneys has occurred. By the time the creatinine is up, a few weeks, months, or years have passed, and now you have a severely scarred kidney.
_
In people with type 1 diabetes, clusters of cells in the pancreas called islets are destroyed. These cells control blood sugar (glucose) levels. Pancreatic islet transplantation is performed in certain patients whose blood glucose levels are especially difficult to control. Tracking the patient’s blood glucose level is the current standard for monitoring islet cell transplant rejection. However, high blood glucose levels are a sign of an advanced stage of rejection. The ability to detect tissue rejection earlier―when fewer cells have been injured―would allow doctors to adjust treatments and help reduce damage to transplanted islets. Many tissues release tiny, fluid-filled sacs called exosomes into the blood and other bodily fluids. These sacs are filled with tissue-specific proteins and genetic material. The scientists analyzed blood samples from 5 people with type 1 diabetes who were enrolled in an islet transplantation clinical trial sponsored by NIH. The team showed that donor islet cell-released exosomes could be reliably characterized throughout a 5-year follow-up period. One patient experienced rejection of the transplanted islets. Researchers detected a decrease in donor cell-exosomes in this patient 6 months prior to an increase in blood glucose. In the 4 patients who didn’t undergo rejection, no decrease in donor cell exosomes was observed. The team also demonstrated that exosomes could be isolated and characterized from urine by analyzing samples from 5 people receiving kidney transplants. These findings suggest that exosomes might one day be used to detect transplant injury earlier than current techniques.
_
Recent studies have highlighted the use of chemokines, cytokines, miRNA, and cells as biomarkers of graft rejection as described in table below:
| Type of rejection | Molecules/cells | Transplant organ | Samples of analysis | Significance | References |
| Acute | CXCL10 | Heart | Blood, serum | Higher serum level of CXCL10 in transplanted patients versus control ones. Among transplanted patients, high expression of CXCL10 is correlated with acute rejection. |
Crescioli et al. 2009 |
| C reactive protein (CRP) | Heart | Blood, serum | Significant differential expression of CRP between rejected and nonrejected heart transplant recipient. In the first year postheart transplantation, CRP was the most useful parameter for noninvasive screening of acute cellular rejection. |
Martinez-Dolz et al. 2009 | |
| Granzyme B CTLA-4 IL-6 TNF-α TGF-β |
Heart | Biopsies | Up-regulation in mRNA expression of all analyzed genes but the strongest increase is seen for granzyme B, TGF-β, and TNF-α genes. Correlation between the expression analysis of these three genes and acute rejection. |
Ramsperger-Gleixner et al. 2011 | |
| CD69 | Heart | Blood, T lymphocytes | Overexpression of CD69 in T lymphocytes of patients with acute rejection. Relationship between increased expression by T lymphocytes and acute rejection is statistically more pronounced for CD8+ T cells than for CD4+ T cells. Presence of CD69+/CD8+ cells exceeding 15% in patients with acute rejection of all T lymphocytes is correlated with vigorous rejection. |
Schowengerdt et al. 2000 | |
| Functional markers of CD4+ T-cell subsets: Th1 Th17 FoxP3+ T cells |
Heart | Blood and biopsies | Higher mRNA expression of the functional markers in patients with acute cardiac rejection in blood and biopsies samples (but not for Th2 mRNA cytokines). Higher percentage of Th1, Th17, and FoxP3+CD4+-circulating T cells. Graft infiltration by Th1 and Th17 cells. Kinetic changes of these CD4+ T-cell subsets after cardiac allograft. |
Wang et al. 2011 | |
| CCL3L1 | Liver | Blood, PBMC | Analysis of copy number variation in genes. Higher number of CCL3L1 gene in patients with acute rejection. |
Li et al. 2012 | |
| Acute | CCL2 CXCL8 CCL5 CXCL9 CXCL10 |
Liver | Blood, serum | Chemokines screening using Luminex multiplex assay. Higher expression of molecules correlated with an up-regulation of NF-κB: CCL2, CCL5, and CXCL8. Higher expression of molecules correlated with T-cell immunity: CXCL9 and CXCL10. Biomarkers of early allograft dysfunction. |
Friedman et al. 2012 |
| Granzyme B Perforin |
Liver | Biopsies | Analysis by immunohistochemistry. Higher frequencies of perforin and granzyme B expression in acute rejection patients. In most of the biopsies, perforin and granzyme B are simultaneously expressed. |
Ji et al. 2004 | |
| Granzyme B | Liver | Biopsies | Higher granzyme B mRNA expression in the biopsies of the acute rejection group. | Krams et al. 1995 | |
| Three subsets of T cells: CD4+CD7+ CD8+CD38+ CD4+CD25+ |
Liver | Biopsies and blood | Higher number of CD4+CD7+ and CD8+CD38+ cells in blood and liver of liver recipient with acute rejection. Decreased expansion of Treg cells (CD4+CD25+) in blood and liver in patients with acute rejection. |
Perrella et al. 2006 | |
| Hepatocyte-derived miRNAs (HDmiRs) | Liver | Blood, serum | Serum level of HDmiRs (miR-122, miR-148a, and miR194) are elevated up to 20-fold in patients with acute rejection. HDmiRs are promising candidates as biomarkers rejection, but also as hepatic injury, after liver transplantation. |
Farid et al. 2012 | |
| CCL4 | Lung | Blood, PBMC | Analysis of copy number variation in genes. Higher number of CCL4 gene in patients with acute rejection. |
Colobran et al. 2009 | |
| Treg and cytotoxic markers | Lung | Bronchoalveolar lavage and blood | Higher mRNA expression for all of the markers in patients with acute rejection, but the expression is significantly increased only for CTLA-4, FoxP3, and granzyme B mRNA. But no differences have been observed in blood samples. |
Madsen et al. 2010 | |
| CD4+/CD8+ T cells NK NK-like T cells B cells Tregs Invariant receptor NK-T cells (iNKT) |
Lung | Bronchoalveolar lavage fluid | Reduction of CD4:CD8 T-cell ratio in patients with acute lung rejection. Higher frequency of CD4+ T cells expressing CD38 during rejection. Proportions of NK and Treg, as a frequency of total CD3+ T cells, trended toward being reduced in rejection. Proportions of B cells, NK-like T cells, and the percentage of CD4−/CD8− iNKT cells trended toward being increased in rejection. |
Gregson et al. 2008 | |
| Acute | CD4+/CD8+ T cells B cells Memory T cells |
Lung | Bronchus-associated lymphoid tissues | Reduction of CD4:CD8 T-cell ratio is correlated with elevated acute rejection episode for patients in the first year of transplantation. | Shenoy et al. 2012 |
| CXCR1 CXCR2 |
Kidney | SNP genotype | Donor CXCR1-2668 GA/AA genotype is associated with acute rejection in kidney transplantation. | Ro et al. 2011 | |
| CXCL10 CXCL13 |
Kidney | Blood, PBMC | Overexpression of CXCL10 and CXCL13 in PBMC of patients with acute rejection. | Mao et al. 2011 | |
| Granzyme B Perforin FasL |
Kidney | Blood,T lymphocytes | Significant higher perforin mRNA expression in patients with acute rejection. No consistent pattern of granzyme B and FasL expression. |
Shin et al. 2005 | |
| CD69 expression | Kidney | Blood,T lymphocytes | Higher percentages of CD69+ cells in the CD3+ and CD8+ T-cell subsets of patients with acute rejection. Correlation between CD69+CD8+ T cells and acute rejection is the more clinically useful test (based on receiver-operator characteristics). |
Posselt et al. 2003 | |
| CXCL10 | Kidney | Blood, serum | High serum level of CXCL10 is associated with acute risk of graft failure. | Rotondi et al. 2004 | |
| CXCL9 | Kidney | Blood, serum | High level of CXCL9 pretransplantation in recipient patients is a marker of high risk of acute rejection. | Rotondi et al. 2010 | |
| Pattern of cytokines Granzyme B Perforin |
Kidney | Blood, PBMC | High level of proinflammatory cytokines (IL-4, IL-5, IL-6, and IFN-γ) and cytotoxic molecules (perforin and granzyme B) are associated with acute rejection in kidney transplant recipient. | Dugre et al. 2000 | |
| CXCL9 CXCL10 |
Kidney | Urine | Increased expression of CXCL9 and CXCL10 in urine of patients with acute rejection. | Jackson et al. 2011a | |
| Granzyme B Perforin |
Kidney | Urine | Increased mRNA expression of granzyme B and perforin in urine of patients with acute rejection. | Li et al. 2001 | |
| Acute | Perforin Granzyme B FasL PI-9 FoxP3 |
Kidney | Urine | Increased mRNA signature expression in urine of patients with acute rejection. FoxP3 mRNA level is the most accurate and predictive for acute rejection with a sensibility and specificity of 100%. |
Aquino-Dias et al. 2008 |
| miRNAs miR-210 |
Kidney | Urine | Down-regulation of miR-10b and miR-210 in patients with acute rejection (compared with controls). Up-regulation of miR-10a in patients with acute rejection (compared with controls). Expression of miR-210 is only one that changes before and after rejection episode. Low expression of miR-210 is correlated with acute rejection and prediction of long-term of kidney function. |
Lorenzen et al. 2011 | |
| CXCR3 | Kidney | Biopsies | Increase number of CXCR3-positive cells in biopsies from patients with acute rejection and decrease with immunosuppressive treatment. | Hoffmann et al. 2006 | |
| CX3CR1 | Kidney | Biopsies | CX3CR1 intragraft staining is associated with worst outcome. CX3CR1 is expressed by macrophage and dendritic cells in acute rejection. |
Hoffmann et al. 2010 | |
| Pattern of chemokines | Kidney | Biopsies | Increase of inflammatory chemokines and chemokine receptors transcripts during acute rejection: CCL3/CCL5/CXCL9/CXCL10/CXCL11 and CCR5/CCR7/CXCR3. Rejection associated with Th1 polarization. |
Lo et al. 2011 | |
| miRNAs | Kidney | Biopsies | Up-regulation of seven miRNA and down-regulation of 10 miRNA samples of patients with acute rejection. Three samples (overexpressed) are predictive with a high accurancy of acute rejection: miR-142-5p, miR-155, and miR-223. |
Anglicheau et al. 2009 | |
| Chronic | CCR4 | Lung | Blood, PBMC | Reduction of CCR4+ expression on CD4+ memory T cells in patients with chronic rejection. | Paantjens et al. 2011 |
| CXCL9 CXCL10 |
Lung | Bronchoalveolar lavage fluid | Cumulative expression of CXCL9 and CXCL10 in bronchoalveolar liquid is a marker of graft failure. | Neujahr et al. 2012 | |
| Chronic | HNPs (human neutrophil peptides 1–3) | Lung | Bronchoalveolar lavage fluid | High level of HNPs peptides by mass spectrometry in patients who have developed bronchiolitis obliterans syndrome (marker of chronic lung rejection). Validation by enzyme-linked immunosorbent assay (ELISA). Monitoring levels of HNPs can predate the clinical onset of disease up to 15 months. |
Nelsestuen et al. 2005 |
| CCL2 | Kidney | Urine | Early detection of CCL2 in urine is a marker of a development of IF/TA at 24 months. | Ho et al. 2010 | |
| CXCL9 CXCL10 |
Kidney | Urine | Increased expression of CXCL9 and CXCL10 in urine of patients with chronic rejection. | Schaub et al. 2009 | |
| CCR1 RANTES |
Kidney | Biopsies | CCR1 and RANTES promote ongoing IF/TA and are linked to worst outcome. | Dikow et al. 2010 | |
| Immunoproteasome β subunit 10 | Kidney | Blood and biopsies | Immunoproteasome β subunit 10 mRNA expression is specifically up-regulated during chronic active antibody-mediated rejection. | Ashton-Chess et al. 2010 | |
| Tribbles-1, -2, and -3 | Kidney | Blood, biopsies and urine |
______
C1q assay:
The C1q assay assesses the ability of an antigen/antibody complex to bind the first component of complement potentially (but not necessarily) leading to target cell killing. It marries the sensitivity and specificity of flow or Luminex solid phase assays with the functionally relevant capacity to fix complement to define antibodies of clinical significance to human leukocyte antigen (HLA) in solid organ transplantation. Since the first reports in 2011 showing high incidence of early rejection in pediatric hearts, acute rejection and graft loss in pediatric and adult kidneys, and confirmed by a subsequent study of more than 1000 kidney recipients, most reports have shown that C1q correlates significantly with risk of antibody-mediated rejection (AMR) and/or graft loss in kidneys. C1q+ donor-specific antibody (DSA) is more clinically relevant for outcome than IgG+ DSA alone especially when de novo DSA (dnDSA) arises posttransplant.
Application of C1q:
As only ∼50% of IgG+ antibodies are C1q+, antibodies can be stratified based on their complement fixing ability. C1q can be used pretransplant for routine antibody screening and monitoring desensitization to strategically expand the donor pool, and posttransplant for monitoring efficacy of rejection therapies. C1q was never intended to be a standalone method for assessing clinical risk of rejection and/or graft failure. Combined data from C1q and IgG assays (e.g. MFI/subclass/titer) and/or other complement fixing assays (e.g. C3d) provide the most informative picture of individualized risk for the patient both before and after transplant.
______
______
Cellular imaging in detecting transplant rejection:
Cellular imaging is an emerging field in magnetic resonance. The ability to non-invasively detect the trafficking and accumulation of different cell types in vivo has broad implications for both a better understanding of biological processes and the clinical diagnosis and treatment of numerous diseases. Imaging the immune response is one area that has particular promise. The immune response plays an important role in numerous pathological conditions, and the development of a robust cellular imaging technique may be broadly applicable across many diseases. Phagocytes, such as macrophages, are readily labelled with a wide variety of MRI detectable agents, and MRI is an excellent modality for anatomical and functional imaging. It is not limited by field of view, depth, or orientation of the target organ, and provides excellent soft-tissue contrast.
_
Cellular MRI has the potential to make a significant impact in detecting organ rejection following transplantation. Despite advances in donor-recipient matching and immunosuppressive drug maintenance therapies, acute rejection remains a threat for graft loss and patient mortality. Monitoring the status of a transplanted organ, such as a heart or kidney, relies heavily on tissue biopsy, an invasive procedure with the associated risks of perforation, bleeding, and infection. Additionally, this procedure is far from ideal because only a few small samples from limited areas are used to determine the status of the whole organ. As a result, mismatch between biopsy results and actual organ rejection status can occur.
_
Using rodent models of organ rejection, researchers have been developing non-invasive, MRI-based methods for detecting and staging graft rejection. They have shown that iron-oxide-based MRI contrast agents, such as nanometer-sized dextran-coated ultrasmall superparamagnetic iron-oxide (USPIO) or micron-sized (MPIO) particles, are excellent cellular contrast agents and provide significant T2-based MRI contrast of macrophage infiltration in models of acute renal rejection as well as acute and chronic cardiac rejection in rats. Perfluorocarbon-based emulsions are a class of agents for cellular MRI that have gained attention in recent years. A key feature of this approach is that once the target cells become labelled, the 19F MRI signal provides a unique marker for cell tracking, with no background signal from the host tissue. The labelled cells can then be placed in their corresponding anatomical context with a conventional 1H image. In conclusion, cellular MRI of in vivo labelled immune cells offers a non-invasive approach to detect and monitor graft rejection after solid organ transplantation. Clinical application of a reliable and non-invasive technique to detect the early signs of graft rejection will improve not only the therapeutic treatment of transplant patients but also improve their quality of life.
______
______
Gene Expression Profiling in Organ Transplantation:
Huge effort is being made among the transplant community investigating novel biomarkers that enable transplant clinicians to identify patients at risk for allograft rejection or those who will develop tolerance so that immunosuppression could be safely minimized or even ideally withdrawn. Despite the important advances achieved in the identification of several potential biomarkers of tolerance, rejection, or both, validation and demonstration of their clinical utility still needs to be tested, which will need international cooperative networks. The search for biomarkers of tolerance or rejection has been focusing at different biological levels, including analysis of sera looking for alloantibodies, peripheral blood mononuclear cells (PBMCs) using different techniques (flow cytometry, microarrays, and reverse transcription PCR), analysis of the urine at the protein, peptide or transcriptomic level, histological assessment of transplant biopsies, and, finally, functional assays measuring alloreactive or antiviral PBMC responses.
_
Non-invasive sources such as peripheral blood have increasingly been targeted to provide information in the field of organ transplantation. Recipient gene expression is profoundly altered after graft implantation. Some of these changes are characteristic of rejection injury. The biological function of the expressed genes encompasses major biological categories of cellular processes related to immune signal transduction, cytoskeletal reorganization, and apoptosis and emphasizes the participation of the cytokine-activated Jak-Stat pathway and interferon signaling in lymphocyte activation proliferation, chemotaxis, and adhesion. Because of the relatively easy induction of permanent renal allograft acceptance in mice with minimal amount of immunosuppression, some groups have assessed the expression of certain genes during either rejection or permanent graft acceptance both in peripheral blood and within the graft tissue. Interestingly, the assessment of two particular gene fragments such as tolerance-associated gene-1, a mitochondrial protein T-cell apoptosis (TOAG-1), and a-1,2-mannosidase (relevant gene for the N-glycosylation of membrane bound and secreted proteins) in a model of kidney and cardiac rat transplantation was shown to be downregulated both in peripheral blood and within the kidney graft prior and during acute and chronic rejection and highly expressed during induction and maintenance of graft acceptance with high specificity and reproducibility. The development of high microarray technology—by assessing changes in expression of multiple genes and quantitation of proteins within human cells, plasma, or tissues—will provide the opportunity for novel insight into molecular pathways of tissue injury and disease processes. Recently, the diagnostic sensitivity, specificity, and accuracy of histological diagnosis using this technology have been improved and both biomarker panels and individual biomarkers have been identified within the allograft to improve the diagnostic, prognostic, and potentially therapeutic categorization of acute rejection.
_
It is important to note that the reproducibility of differently expressed genes might be affected by many factors such as gene ranking and selection methods, inherent differences between types, and the choice of thresholds. However, because microarray analyses are expensive and time consuming and their statistical evaluation is often very difficult, gene expression analysis using the RTPCR method is nowadays recommended. In the field of organ transplantation, gene-expression-based decision might help in improving patient and graft outcome and there are a multitude of studies showing that gene-expression profiling is feasible.
_
DNA microarray analysis to measure changes in the levels of gene expression:
Analysis of gene expression using genomic microarrays can complement clinical research and may provide insights into disease pathogenesis. A microarray is a high-throughput technology that consists of a series of small nucleic acid sequences or oligonucleotides (called probes) that are attached to a solid surface (i.e. glass slide or a silicon chip). Millions of probes can be contained in one array. DNA and RNA of experimental and/or control samples can be extracted, labelled, and hybridized to the probes under high-stringency conditions. Probe–target hybridization is usually detected and quantified by fluorescence-based detection methods to determine relative abundance of DNA sequences in the target (ratio of test to reference sample). DNA microarrays can be used to measure changes in the levels of gene expression or to detect single nucleotide polymorphisms. The technology is reproducible across multiple samples and when large numbers of genes are analyzed, it can be used to identify patterns of gene expression within disease states that are believed to correlate with functional changes at the protein level. This technology can produce an overwhelming amount of data that must be analyzed using sophisticated data analysis software. The current cost and complexity of this technology precludes its use as a screening tool in the clinical setting.
_
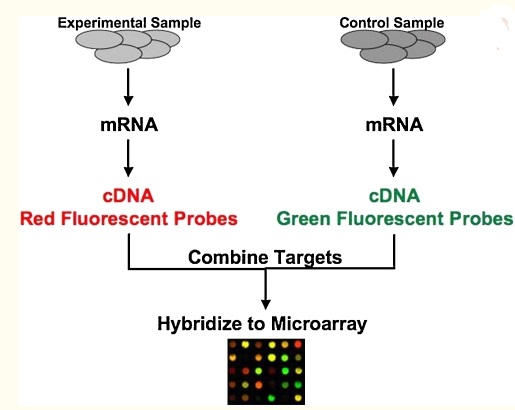
Figure above shows DNA from experimental samples is purified and fluorescently labelled and then hybridized to immobilized probes on the array to determine alterations in gene expression
_
DNA microarrays have been applied to peripheral blood and renal allograft biopsy samples of pediatric patients with and without graft dysfunction in the posttransplant period. Several gene expression patterns are altered during acute rejection episodes, chronic allograft nephropathy, and infection. Three molecular categories have been identified during acute rejection episodes that appear to correlate with graft function and survival. For example, biopsy samples that demonstrate enhanced B cell-related genes appear to have the worst outcomes. Since this initial study, many studies have subsequently been performed in both humans and mice investigating acute rejection, chronic allograft nephropathy, operational tolerance, minimum immunosuppression, infections, and drug toxicity. In some cases, these have resulted in the identification of molecular subtypes that can predict outcome and response to treatment; in other cases, potential novel therapeutic targets have been identified. The expectation from these studies is to move from a ‘one-size fits all’ to a more personalized approach to posttransplant immunosuppressive regimens.
______
______
Donor DNA circulating in the recipient’s plasma in transplant rejection:
It is challenging to monitor the health of transplanted organs, particularly with respect to rejection by the host immune system. Because transplanted organs have genomes that are distinct from the recipient’s genome, researchers used high throughput shotgun sequencing to develop a noninvasive approach to monitoring organ health. They analyzed cell-free DNA circulating in the blood of heart transplant recipients and observed significantly increased levels of cell-free DNA from the donor genome at times when an endomyocardial biopsy independently established the presence of acute cellular rejection in these heart transplant recipients. Their results demonstrate that cell-free DNA can be used to detect an organ-specific signature that correlates with rejection, and this measurement can be made on any combination of donor and recipient. This noninvasive test holds promise for replacing the endomyocardial biopsy in heart transplant recipients and may be applicable to other solid organ transplants.
![]()
Instead of monitoring the recipient’s immune response, researchers have developed an assay that directly interrogates the health of the donated organ. This technique involves measuring the signature of dying cells from the organ in the cell-free DNA circulating in the recipient’s plasma. If a unique genomic signature of DNA from the donated organ (compared with the recipient’s genome) can be identified, then the level of “donor DNA” from the transplanted organ can be monitored over time, and changes in organ health can be detected as changes in the donor DNA level. The rationale for this approach arises from the observation that both acute and chronic rejection processes are associated with apoptosis of specific cell types within the allograft.
Past research has attempted to identify cell-free DNA in sex-mismatched female recipients of male donor organs, where chromosome Y can serve as the donor genetic signature. This line of research, however, has yielded conflicting results on the existence of a donor-specific signature in the plasma of organ transplant recipients. The clearest evidence has come from renal transplantation, where donor-specific chromosome Y has been detected in recipient urine and plasma. To date, most measurements of cell-free DNA in organ transplantation have been limited to the special case of women who receive male organs, which has prevented the widespread use of cell-free DNA as a diagnostic tool, because female recipients of male donor organs represent less than a quarter of all transplant procedures. HLA markers can be quantified to identify donor-derived DNA in pancreas–kidney transplant recipients, but the precision is low, making its utility to measure rejection unclear, and it is not applicable to cases when the donor and recipient are HLA matched.
_
Donor DNA from healthy transplant vs. transplant in rejection:
![]()
Figure above shows that Cell-free DNA collected in plasma contains a majority of molecules from the recipient (in gray) but may also include some from the transplanted organ (green). Due to increased cell death in the organ during a rejection episode, more donor molecules are expected to be present in the blood at these times. Shotgun sequencing of the purified DNA allows for counting recipient versus donor molecules by looking at single nucleotide polymorphisms (SNPs) that vary between donor and recipient. Very high levels of donor DNA, particularly changes from past measurements, will indicate the onset of rejection. Here, researchers show that organ-specific donor DNA is detectable in the plasma of heart transplant recipients and that this genetic signature increases substantially before rejection events. They also demonstrate a universal, sex-independent strategy using shotgun sequencing to measure single nucleotide polymorphism (SNP) differences between individuals to quantify the donor DNA signal. This genome transplant dynamics (GTD) approach is applicable to any organ donor and any recipient, regardless of sex, by first genotyping the donor and recipient to establish a unique donor “genetic fingerprint,” which can be detected by high throughput sequencing of cell-free DNA in the recipient’s blood following transplantation. The GTD assay provides a quantitative measure of organ health that can complement or possibly replace other approaches for posttransplant monitoring.
_
When the patients were healthy and rejection was under control, less than 0.5 percent of the DNA detected in the blood was from the donor heart. The study found that above a threshold of two percent donor DNA in the blood, there was an 80 percent true positive rate for tissue rejection, along with a 15 percent false positive rate. They were also able to demonstrate an increase in the amount of donor DNA detected over time before the onset of rejection symptoms, which other techniques under consideration have not been able to accomplish. Because donor DNA can be detected earlier than other rejections signals, physicians might use that information to increase immune suppression to get ahead of a rejection event before it happens, keeping both the transplanted organ and the patient recipient healthier.
_____
_____
Prevention and treatment of transplant rejection:
When a patient receives a heart, lung, liver, kidney, or pancreas from an organ donor (living or deceased), the patient’s immune system will recognize the foreign tissue and mobilize to reject the organ unless he or she takes medications that suppress the immune system’s natural processes. These medications, known as immunosuppressants, are a lifelong requirement after organ transplantation. While these drugs allow people to tolerate the presence of foreign organs, they also increase patients’ risk of contracting infections, and cancers and are associated with other undesirable side effects. Over the years since organ transplants were first done, these medicines have greatly improved. Researchers are finding out more all the time about how to better regulate the immune system after a transplant. Current medicines still have the potential to speed up illness or create new disease, such as heart problems, diabetes, cancer, and osteoporosis. But these medicines also will save your life by keeping your body from rejecting the donor organ. It is important to take these medicines daily and exactly as prescribed. Taking medicines daily for the rest of your life is not as hard as it sounds. It may help to talk to someone who has had a transplant and who can assure that you will be able to make the medicines a part of your daily routine. Over time, probably, fewer medicines will be needed. Additional medicines may be needed now and then to fight infection or other health problems related to your transplant.
_
History of immunosuppressant:
The ability to prolong life by transplanting organs had long been a dream of medical practitioners. Early efforts at transplantation were unsuccessful because of inadequacies in surgical technique and lack of fundamental knowledge of the immune system. Skin and eyes were among the first successful transplants. However, the more complex organs posed countless problems. The kidney was the first such organ to be successfully transplanted. Surgical techniques progressed with the unsuccessful attempt at transplanting a cadaveric kidney in 1933. Initial attempts at immunosuppression were with total body radiation, but all the patients died. Steroids alone were then used, also without success. With the development of 6-mercaptopurine, followed by azathioprine in the early 1960s, pharmacological immunosuppression became the standard of care. In the early 1960s, 2 major breakthroughs finally addressed the rejection problem. Beginning in 1962, it became possible to closely match donor and recipient tissue. After the first initially successful series of transplantations performed between 1962 and 1964, the combination of azathioprine and steroids came into widespread use and became part of the primary immunosuppressive regimen for the next 20 years. As knowledge of the immune system evolved, therapy targeted to specific immunoregulatory sites became possible. The first polyclonal antilymphocyte globulin was used in 1967 and spawned the development of other polyclonal and monoclonal antibodies. Introduced in the 1980s, cyclosporine, a calcineurin inhibitor, was used in combination with azathioprine and steroids and was credited with a dramatic improvement in graft survival. Cyclosporine greatly improved the outcome of such transplants. The first successful heart-lung transplant was carried out in 1981. The next advance came in 1994 with the introduction of mycophenolate mofetil. After tacrolimus (another calcineurin inhibitor) became available in 1994, debate followed regarding which calcineurin inhibitor was superior. Tacrolimus has gradually supplanted cyclosporine in many centers. In contrast, mycophenolate mofetil rapidly replaced azathioprine almost universally. To expand the armamentarium further, sirolimus, a macrolide antibiotic, was developed and released. While the short-term outcomes provided with these medications have continued to improve, the consequences of their administration have become the subject of intense scrutiny as comorbid conditions, drug toxicities, and adverse effects keenly affect both patient and graft survival.
_
Immunosuppressants are a class of drugs that suppress the immune response through various mechanisms. In organ transplantation, immunosuppressants are used to prevent the body from either recognition or attacking the foreign organ via various immune responses. They should only be used under the supervision of appropriately trained and experienced staff.
Immunosuppressants in organ transplant are used for:
- Preventing organ rejection and reverse acute rejection in organ transplantation.
- Prevent and treat graft-versus-host disease.
- Minimise destruction of affected tissues in autoimmune and inflammatory diseases.
Transplant rejection involves the body producing T and B cell and immune responses that recognise markers on foreign tissue called antigens. Treatment regimens used to prevent rejection employ drugs from different classes taking advantage of their complementary actions and minimising toxicity. Drug choice depends on the organ being transplanted and is tailored for each individual to minimise transplant-related morbidity.
_
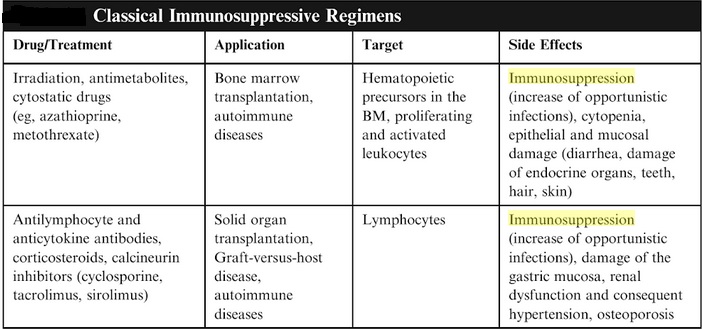
Immunosuppression after solid organ transplantation is complex. Over the past 50 years, the medical community has witnessed great advances in the care of patients receiving organ transplants. Improved therapeutic strategies have been associated with better patient and graft survival rates; however, the adverse effects associated with these agents and the risks of long-term immunosuppression present a number of challenges for the clinician. With all the successes of immunosuppressive therapies come the obligations to tailor treatments to meet the individual patient’s characteristics and to balance the risks and benefits of these medications. The use of any immunosuppressive drug requires a balance between the risk of loss of transplanted organ and the toxicity of the agent. The goal is to balance an appropriate level of immunosuppression with the long-term risks, which include development of infections, cancer, and metabolic complications.
_
The figure below depicts the points of action of immunosuppressive drugs:
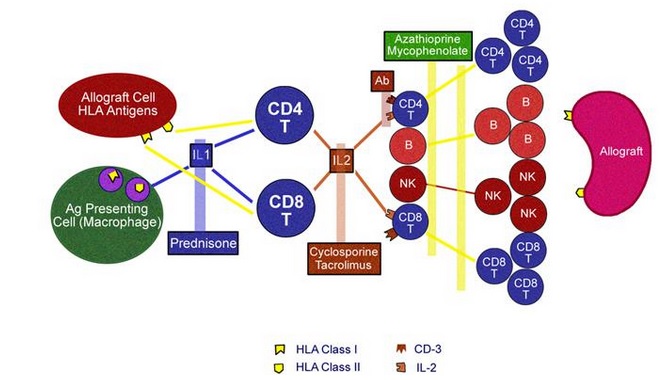
Figure above illustrates the points of action of immunosuppressive drugs. Corticosteroids inhibit production of interleukin-1. Macrolides (i.e., cyclosporine, tacrolimus, sirolimus) inhibit production of or use of interleukin-2, thus inhibiting stimulation of a clone of cytotoxic T lymphocytes directed against specific human lymphocyte antigen types. Antimetabolites (i.e., mycophenolate mofetil, azathioprine) inhibit purine production, thus impairing cell proliferation. Antibodies impair normal function of cell surface markers, thus inhibiting stimulation of T-lymphocyte clones directed against foreign antigens.
_
Corticosteroids:
Corticosteroids are used for induction and maintenance immunosuppression, as well as for acute rejection. These agents prevent production of cytokines and vasoactive substances, including interleukin (IL)–1, IL-2, IL-6, tumor necrosis factor-α, chemokines, prostaglandins, major histocompatibility class II, and proteases. Corticosteroids act as agonists of glucocorticoid receptors but, at higher doses, have receptor-independent effects. Glucocorticoid receptors are in cytoplasm in an inactive complex with heat shock proteins. The binding of corticosteroids to the glucocorticoid receptors dissociates heat shock protein from the glucocorticoid receptor. Formed active corticosteroid–glucocorticoid receptor complex migrates to the nucleus and dimerizes on palindromic DNA sequences in many genes. The binding of glucocorticoid receptors in the promoter region of the target genes can lead to either induction or suppression of gene transcripts. The most common corticosteroids used in transplantation are oral prednisolone and intravenous methylprednisolone. These agents are metabolized by the liver and excreted by the kidneys as inactive metabolites. Drug interactions with P450 inhibitors and inducers are common.
Adverse effects of corticosteroids include cushingoid features, osteoporosis, avascular necrosis, cataracts, glucose intolerance, infections, hyperlipidemia, hypertension, peptic ulcer disease, pancreatitis, bowel perforation, weight gain, psychiatric disturbances, and growth restriction. Orofacial clefts and fetal adrenal suppression with corticosteroids have been reported in pregnancy.
_
Calcineurin inhibitors:
- Cyclosporine:
Cyclosporine has been a keystone of immunosuppression in transplantation for 4 decades. This agent is used for induction and maintenance immunosuppression. Cyclosporine inhibits T cell proliferation by blocking activation. When foreign peptide antigen is presented to the recipient’s T cell, binding to the antigen-binding groove of the major histocompatibility complex (MHC) triggers activation of the T cell. The rate-limiting step in the activation cascade is a serine–threonine phosphatase called calcineurin. When cyclosporine enters a lymphocyte, it binds to an immunophilin called cyclophilin. This cyclosporine–cyclophilin complex inhibits calcineurin and so arrests T cell activation. Cyclosporine is a polypeptide of 11 amino acids of fungal origin and a prodrug that binds to cyclophilin; complex inhibits calcineurin phosphatase and T-cell activation by dephosphorylation of inactive nuclear factor of activated T cells (NF-AT). Therefore, it prevents the production of IL-2 via calcineurin inhibition. Cyclosporine trough level or checking levels 2 hours after administration is required. Multiple drug interactions are possible, primarily with agents affecting the cytochrome P-450 system.
Adverse effects of cyclosporin include nephrotoxicity (immediate, secondary to renal ischemia; 2-3 weeks after transplantation, secondary to renal vasoconstriction; and chronic, secondary to interstitial nephritis). Other adverse effects include hyperkalemia, hypomagnesemia, nausea, vomiting, diarrhea, hypertrichosis, hirsutism, gingival hyperplasia, skin changes, hyperlipidemia, glucose intolerance, infection, malignancy, hyperuricemia, and hemolytic uremic syndrome. Hypertrichosis and hirsutism can be alleviated by switching from cyclosporine to tacrolimus. The adverse consequences (e.g., hypertension, renal impairment) of long-term cyclosporine use for solid organ transplant rejection have prompted exploration of various treatment regimens.
- Tacrolimus:
Tacrolimus is a macrolide antibiotic and is active against helper T cells, preventing the production of IL-2 via calcineurin inhibition (binds to tacrolimus-binding protein instead of cyclophilin protein). The tacrolimus:FKBP12 active complex inhibits calcineurin with greater potency than the corresponding cyclosporine complex. This agent is used for maintenance immunosuppression and for rescue therapy in patients with refractory rejection under cyclosporine-based therapy. Multiple drug interactions are possible, primarily with agents affecting the cytochrome P-450 system. One study evaluated the long-term safety and efficacy of tacrolimus in orthotopic liver transplantation (OLT). The study reviewed 1000 primary OLTs performed between August 1989 and December 1992 and maintained with tacrolimus-based immunosuppression therapy. After 17- to 20-year follow-up, the results found patient survival rates at 35.8% and graft survival rates at 32.6%, with significantly better survival among children. Graft loss was attributed to age-related complications, recurrence of primary disease, and malignancy; rarely was graft loss related to immunologic reasons. The data conclude that tacrolimus is a potent immunosuppressive agent in OLT.
Adverse effects are similar to those of cyclosporine but with a lower incidence of hypertension, hyperlipidemia, skin changes, hirsutism, and gum hyperplasia and a higher incidence of new-onset diabetes mellitus after transplantation (NODAT) and neurotoxicity. Although tacrolimus causes less cosmetic effects than cyclosporine, it can cause reversible alopecia.
_
Mammalian target of rapamycin (mTOR) inhibitors:
Sirolimus, also called rapamycin, is a macrolide product of a soil fungus found on Easter Island. This agent is used for maintenance immunosuppression and chronic rejection. Everolimus is a rapamycin analog with a similar mechanism of action and adverse effect profile. The mode of action of sirolimus is to bind the cytosolic protein-FKBP12 in a way similar to tacrolimus. Unlike the tacrolimus-FKBP12 complex, which inhibits calcineurin, the sirolimus-FKBP12 complex inhibits the mTOR pathway by directly binding the mTOR Complex1 (mTORC1). This complex inhibits signal 3 by stopping translation of the RNA and preventing the progression from G1 phase to the S phase of DNA synthesis. It also inhibits IL-2– and IL–4-dependent proliferation of T and B cells. Similarly, sirolimus inhibits proliferation of nonimmune cells and the pathways that could be involved in oncogenesis. The antiproliferative effects of sirolimus may have a role in treating cancer. Sirolimus was shown to inhibit the progression of dermal Kaposi sarcoma in patients with renal transplants. Sirolimus-based regimens have been associated with a reduced incidence of posttransplantation malignant neoplasms. It has been reported that a cyclosporine a–free immunosuppressant regimen based on sirolimus reduced aortic stiffness, plasma endothelin-1, and oxidative stress in renal transplant recipients enrolled in the CONCEPT trial.
Multiple drug interactions are possible, especially because of the extremely long half-life. Concomitant use with strong CYP3A4/P-gp inducers or strong CYP3A4/P-gp inhibitors decreases or increases sirolimus concentrations. When mTOR inhibitors are used simultaneously with cyclosporine, maximum concentration of the drug (Cmax) and area-under-the-curve (AUC) for both the compounds are increased. Thus, it is recommended that cyclosporine and mTOR inhibitors to be administered 4 hours apart. Extensive experience in clinical renal transplantation has resulted in successful conversion of patients from calcineurin inhibitors to mTOR inhibitors at various times post-transplantation, with excellent long-term graft function. Widespread use of this practice has, however, been limited owing to mTOR-inhibitor- related toxicities. Unique attributes of mTOR inhibitors include reduced rates of squamous cell carcinoma and cytomegalovirus infection compared to other regimens. Adverse effects associated with mTOR inhibitors are hyperlipidemia, thrombocytopenia, anemia, pneumonitis, oral ulcers, and diarrhea. Low testosterone levels may cause infertility. These agents can also cause poor wound healing and dehiscence formation of lymphoceles. When used combination with calcineurin inhibitors, sirolimus potentiates calcineurin nephrotoxicity. Sirolimus is associated with worsening of proteinuria. It may also cause delayed recovery from acute tubular necrosis. Although successful pregnancies with sirolimus have been reported, it is not routinely used in pregnancy. Finally, thrombotic angiopathy cases have been reported with sirolimus. Avoidance of calcineurin may be considered in patients with a primary etiology of atypical hemolytic uremic syndrome or other forms of thrombotic angiopathy, and use of sirolimus may “decrease” the incidence of hemolytic uremic syndrome recurrence.
_
Inhibitors of nucleotide synthesis (purine synthesis inhibitors):
- Mycophenolate acid:
Mycophenolic acid (MPA) is the active component of mycophenolate mofetil and mycophenolate sodium. MPA blocks inosine monophosphate dehydrogenase (IMDH), an enzyme required for the de novo synthesis of guanosine nucleotides. While other cells have salvage pathways by which guanosine nucleotides may be synthesized, lymphocytes do not. MPA thus blocks lymphocyte proliferation by blocking DNA synthesis. This agent is used for maintenance immunosuppression and chronic rejection. It is more potent than azathioprine and is associated with a greater reduction in acute rejection; however, it is not as potent as mTOR or CNIs, and is generally used in combination with one of those drug classes. Adverse effects include nausea, vomiting, diarrhea, leukopenia, anemia, and thrombocytopenia.
In current practice, tacrolimus and mycophenolate mofetil are considered more efficient than cyclosporine A and mycophenolate mofetil, but recent studies have challenged this assumption. With antithymocyte globulins and steroids, clinically suspected acute rejections did not differ between cyclosporine A//azathioprine and tacrolimus/mycophenolate mofetil arms. Cyclosporine A/azathioprine allowed a low acute rejection rate, but tacrolimus/mycophenolate mofetil seemed to be a better regimen regarding severe secondary outcomes.
Among a cohort of patients being followed long term, mycophenolate mofetil appeared to be highly efficient for preventing both allograft rejection episodes and the development of coronary artery stenoses early after heart transplantation. Mycophenolate mofetil also significantly improved the survival of heart transplant recipients compared with azathioprine, despite a greater incidence of infections linked to mycophenolate mofetil therapy. A study from the National Adult Solitary Renal Transplant Recipients database from 1998 to 2006 evaluated patient death and graft loss, complications, and renal function. One-year acute rejection rates were reduced for patients on mycophenolate mofetil versus azathioprine (10% vs. 13%, P < .01); there were no statistically significant differences for malignancies, renal function, or BK virus infection at 1 year. The primary findings suggested that the association of mycophenolate mofetil with improved outcomes may not be apparent in patients also receiving tacrolimus.
Enteric-coated mycophenolate sodium (EC-MPS):
EC-MPS is introduced with fewer reports of gastrointestinal adverse effects. Acute noninfectious diarrhea after simultaneous pancreas and kidney transplantation is related to the duration of diabetes and to prescription of mycophenolate mofetil, a prodrug of mycophenolate acid. Preferential use of EC-MPS is associated with a lower necessity of dose reduction and less severe episodes of acute diarrhea compared with mycophenolate mofetil, although dose reduction is equally associated with acute episodes of kidney rejection.
- Mizoribine:
Mizoribine has been demonstrated to inhibit T-lymphocyte proliferation by depleting these cells of guanine ribonucleotides as a consequence of inhibiting the enzyme IMDH. Inhibition of guanine ribonucleotide biosynthesis appears to be a novel and perhaps more selective mechanism of inhibiting T-cell proliferative responses after T-cell activation. Its use has not been approved in North America. It has been used widely in Japan. Multicenter, randomized clinical trials revealed that the efficacy and safety of mizoribine were similar and statistically not inferior to mycophenolate mofetil in combination therapy with tacrolimus. The uric acid level was significantly elevated in the mizoribine group (P = .002). Case reports describe acute kidney injury due to uric acid nephropathy.
_
Leflunomide:
Leflunomide is a synthetic isoxazole-derivative drug that possesses both immunosuppressive and antiviral properties. It has been used off-label in the setting of resistant CMV infection or BK virus nephropathy, or in renal transplant recipients with chronic allograft dysfunction. A prospective randomized trial is needed for its use in transplantation. Its careful usage under close monitoring may provide to eradicate BK virus or CMV infection. Its current use as a first-line agent instead of mycophenolate mofetil or sirolimus cannot be recommended. Adverse effects such as hepatotoxicity and hemolytic anemia cannot be overlooked.
_
Azathioprine:
Azathioprine was the first immunosuppressive agent used in organ transplantation and provided a share of the 1988 Nobel Prize to its developers. It is an antimetabolite prodrug that converts 6-mercaptopurine to tissue inhibitor of metalloproteinase, which is converted to thioguanine nucleotides that interfere with DNA synthesis. Other possible mechanism includes converting co-stimulation into an apoptotic signal. It is used for maintenance immunosuppression; however, it became a second-line drug after cyclosporine was introduced. Adverse effects of azathioprine include leukopenia, thrombocytopenia, and liver toxicity. Myelosuppression becomes a serious problem when used with allopurinol. The dose of azathioprine should be decreased when administered with allopurinol and when withdrawing steroids. Complete blood cell counts and pancreatic and liver enzyme levels must be monitored. Myelosuppression can improve with drug discontinuation. Azathioprine is compatible with cyclosporine and tacrolimus. Azathioprine use in transplantation has been widely replaced by mycophenolate mofetil in North America. Results from a study on the conversion from mycophenolate mofetil to azathioprine in high-risk renal allograft recipients on cyclosporine-based immunosuppression suggest that selective conversion from mycophenolate mofetil to azathioprine after 1 year is safe, even in high-risk kidney transplants. Normal serum creatinine and absence of proteinuria are good screening parameters to identify patients at low risk for acute rejection following such conversion. Cost comparison suggests azathioprine to be 6-10 times cheaper than mycophenolate mofetil. In tacrolimus-based immunosuppression, azathioprine may be as good as mycophenolate mofetil as a maintenance immunosuppressive drug in living-donor kidney transplantation. The 3-year results of a randomized, double-blind, controlled trial of mycophenolate mofetil versus azathioprine in heart transplant patients revealed no significant differences between treatments in quantitative coronary angiographic measurements of transplant coronary vasculopathy. Congestive heart failure, atrial arrhythmia, and leukopenia were more common in the azathioprine group, whereas diarrhea, esophagitis, herpes simplex infection, herpes zoster infection, and CMV infection were more common in mycophenolate mofetil–treated patients. Consideration is increasing on whether mycophenolate acid provides survival benefits comparable to azathioprine after renal transplantation. The type of antimetabolite, azathioprine or mycophenolate acid, was not independently associated with any safety or efficacy outcome 5 years after transplantation, suggesting that azathioprine is still a viable option for low-risk kidney transplantation recipients receiving tacrolimus and steroids.
______
Biologic agents:
Biologic agents are polyclonal and monoclonal antibodies and are frequently used in transplantation for induction immunosuppression or treatment of rejection. The 3 antibodies used for induction therapy are the lymphocyte-depleting agents: (1) antithymocyte globulin, (2) alemtuzumab, and (3) basiliximab. Historically, immunosuppressant selection was based solely on efficacy for the prevention of rejection. In the current era of transplantation, it is now common practice in the transplant community to select induction therapy based on risk-benefit considerations for each patient.
_
- Polyclonal antibodies (antithymocyte globulins ATG)
Antithymocyte globulins have been used commonly for induction immunosuppression and treatment of acute rejection in solid organ transplantation. These agents are derived by injecting animals (rabbit or horse) with human lymphoid cells, then harvesting and purifying the resultant antibody. Polyclonal antibodies induce the complement lysis of lymphocytes and uptake of lymphocytes by the reticuloendothelial system and mask the lymphoid cell-surface receptors. Preparations include horse antithymocyte globulin (Atgam) and rabbit antithymocyte globulin (Thymoglobulin, ATG). Although ATG is the favored agent, equine preparations have historically been used. Most regimens involve 5-7 days of intravenous administration of thymoglobulin for induction immunosuppression or treatment of corticosteroid-resistant rejection or antibody-mediated rejection. Thymoglobulin is a polyclonal antibody that has been used in the field of transplantation over the last 4 decades. Thymoglobulin’s lack of nephrotoxic properties (unlike calcineurin inhibitors) may potentiate it to be a beneficial induction therapy during the early days following transplantation. In conjunction with inhibitors of terminal complement activation, it has been shown to be beneficial in cross-match–positive transplantation. Thymoglobulin possibly provides better protection against acute rejection and improves patient and graft survival but may result in more CMV infection and posttransplantation malignancy. Thymoglobulin causes leukocyte depletion with a greater delay to recover. Of special importance is adding antiviral therapy to the treatment regimen of patients who receive antithymocyte globulins as induction therapy. As polyclonal agents are xenogenic proteins, adverse effects include fever and chills. Other adverse effects are thrombocytopenia, leukopenia, hemolysis, respiratory distress, serum sickness, and anaphylaxis. Thymoglobulin rarely causes adult respiratory distress syndrome. Some adverse effects are ameliorated with steroids, acetaminophen, and diphenhydramine. A high average dose of antithymocyte immunoglobulin has been associated with an increased risk of non-Hodgkin lymphoma. Thymoglobulin administration is associated with coagulopathy. Using an international normalized ratio screening protocol and an aggressive transfusion protocol, bleeding complications associated with coagulopathy can be avoided in this higher-risk group.
_
- Murine monoclonal anti-CD3 antibody (muromonab-CD3):
Muromonab-CD3 (OKT3) is a murine monoclonal antibody of immunoglobulin 2A clones to the CD3 portion of the T-cell receptor. It blocks T-cell function and has limited reactions with other tissues or cells. This agent is used for induction and acute rejection (primary treatment or steroid-resistant). Soon after muromonab-CD3 administration, T cells disappear from the circulation as a result of opsonization and subsequent removal by the reticuloendothelial system. Adverse effects include cytokine release syndrome (i.e., fever, dyspnea, wheezes, headache, hypotension) and pulmonary edema. Avoiding administration in hypervolemic patients is especially important, although pulmonary edema can occur in euvolemic patients. This therapy requires premedication with steroids (first 2 doses only), acetaminophen, and diphenhydramine to avoid cytokine release syndrome. Its effects of therapy can be monitored by using a CD3 antigen assay. Muromonab-CD3 is immunogenic in humans, and approximately 50% of patients make antibodies to it after a course of treatment, decreasing the efficacy of subsequent courses. Post transplantation lymphoproliferative disorders have been reported after muromonab-CD3 administration.
_
- Humanized monoclonal anti-CD52 antibody (alemtuzumab):
Alemtuzumab, a humanized monoclonal antibody directed against CD52, is a lymphocyte-depleting agent currently being evaluated as an induction agent in solid organ transplantation. Alemtuzumab has been used in off-label studies of solid organ transplantation. CD52, a 25- to 29-kd membrane protein and is on all B and T cells and most macrophages and natural killer cells. Alemtuzumab has powerful depletional properties and a favorable cost profile compared with other induction agents. Treatment results are a rapid and effective depletion of lymphoid cells that may take several months to return to pretransplantation levels.
The use of alemtuzumab as induction immunosuppression for renal transplantation introduces the possibility of long-term tacrolimus monotherapy, avoiding maintenance with both corticosteroids and mycophenolate mofetil. Renal transplantation with alemtuzumab induction followed by tacrolimus monotherapy leads to good graft and patient outcomes, with no major differences detected compared with basiliximab induction and tacrolimus/mycophenolate mofetil maintenance at 1 year. It was shown that alemtuzumab induction is associated with delayed inflammation at 4 and 12 months, but this inflammation did not appear to negatively impact the glomerular filtration rate or graft survival.
Adverse effects of alemtuzumab include mild cytokine-release syndrome, neutropenia, anemia, idiosyncratic pancytopenia, autoimmune disorders (e.g., hemolytic anemia), thrombocytopenia, and thyroid disease. Further controlled trials are needed to establish safety and efficacy. The risk of immunodeficiency-related malignancies was evaluated in a retrospective study including 1350 kidney transplant recipients (between 2001 and 2009). The study concluded that with the exception of nonmelanoma skin cancer and after excluding cancers occurring within 60 days posttransplantation, alemtuzumab induction was not associated with increased cancer incidence post kidney transplantation when compared with no induction therapy and was associated with lower cancer incidence compared with thymoglobulin.
_
- Monoclonal anti-CD25 antibody
Basiliximab and daclizumab are chimeric and humanized antimonoclonal antibodies that target the IL-2 receptor (CD25). Clinically, both agents are very similar, and both are used for induction. These agents bind to the IL-2 receptor α-chain (CD25 antigen) on activated T cells, depleting them and inhibiting IL-2–induced T-cell activation. Daclizumab was withdrawn from the United States market because of diminished use and emergence of other effective therapies. These agents have a very low prevalence of adverse effects, although hypersensitivity reactions have been reported with basiliximab, albeit rarely. Induction treatment with basiliximab requires 2 doses, and no monitoring is required. Induction with daclizumab requires 5 doses but 2 may suffice; no monitoring is required.
_
- Anti-CD20 antibodies
Rituximab (anti-CD20 monoclonal antibody) eliminates most B cells and is approved for treating refractory non-Hodgkin B-cell lymphomas, including some posttransplantation lymphoproliferative disease in organ transplant recipients. Rituximab is used off-label in combination with maintenance immunosuppressive drugs, plasmapheresis, and intravenous immune globulin to suppress deleterious alloantibody responses in transplant recipients. Although plasma cells are usually CD20 negative, many are short-lived and require replacement from CD20-positive precursors. Thus, depletion of CD20-positive cells does reduce some antibody responses. CD20-positive B cells can act as secondary antigen-presenting cells, which raises the possibility that rituximab can ameliorate T-cell responses. Off-label applications for rituximab include treatment of antibody-mediated rejection and possibly severe T-cell–mediated rejection and suppression of preformed alloantibody before transplantation. Again, controlled trials are needed. Antibody-mediated rejection is a major cause of late kidney transplant failure. Although plasmapheresis is effective in removing alloantibodies (donor-specific antibodies) from the circulation, rebound synthesis of alloantibodies can occur.
_
- Splenectomy is used in desensitization protocols for ABO-incompatible transplants and for antibody-mediated rejection refractory to conventional treatment. Also used are agents targeted for plasma cells, B cells, and the complement cascade, which are bortezomib, rituximab, and eculizumab, respectively.
_
- LEA29Y:
LEA29Y is a second-generation cytotoxic-T-lymphocyte–associated antigen 4 (CTLA-4) immune globulin that is a fusion protein combining CTLA-4 (which engages CD80 and CD86) with the Fc portion of immunoglobulin G. The LEA29Y trial introduces the concept of long-term use of nondepleting protein immunosuppressive agents to reduce reliance on toxic small-molecule immunosuppressive drugs.
_
- Many new agents are designed to interfere with secondary signalling, and this may aid in induction of tolerance.
Monoclonal antibodies to B7-1 (CD80) and B7-2 (CD86) have been developed to block T-cell CD28 activation and proliferation responses. In a recent trial, one of these antibodies, belatacept, did not appear to be inferior to cyclosporine as a means of preventing acute rejection after renal transplantation. Studies involving the humanized anti-C5 antibody, eculizumab, have demonstrated the effects of a new antibody therapy on the prevention of antibody-mediated rejection in highly sensitized patients who undergo transplantation. In 2014, eculizumab was granted orphan drug designation for the prevention of delayed graft function in renal transplant patients.
_____
Immunosuppressant medications interactions:
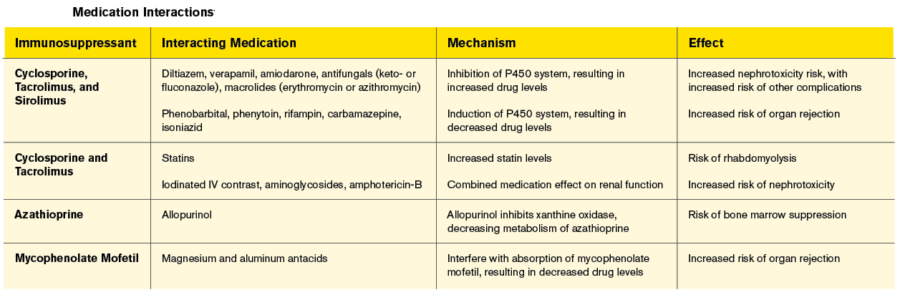
_____
_____
Therapeutic Management:
Immunosuppressive drugs can be classified as induction therapies, maintenance therapies and antirejection therapies. Immunosuppressive treatment of the transplantation patient begins with the induction phase, perioperatively and immediately after transplantation. Maintenance therapy then continues for the life of the allograft. Induction and maintenance strategies use different medicines at specific doses or at doses adjusted to achieve target therapeutic levels to give the transplantation patient the best hope for long-term graft survival.
Phases:
- Induction prophylaxis (prevention) (induction therapy) is a course of intensive immune suppression for about 2 weeks immediately post transplantation and is often started immediately pre-operatively with the aim of ‘switching off’ the immune system after transplantation. Initial prophylaxis (prevention) (initial therapy) is the treatment given to all recipients (except where donor is an identical twin) for 0-3 (sometimes up to 6) months after transplantation.
- Maintenance prophylaxis (prevention) (maintenance therapy) is the treatment that patients receive long-term, throughout the duration of allograft survival.
- Acute rejection treatment is the therapy following acute rejection and especially following multiple rejection episodes. Resistant rejection treatment is a therapy of acute rejection resistant to high dose glucocorticosteroids during a defined period of time.
_
Immunosuppression for organ transplants usually involves triple or quadruple drug treatment. The intensity of immunosuppression is initially high but tends to be reduced to a maintenance level that is determined by individual factors and the type of organ transplant.
Quadruple therapy: Usually: (1) induction therapy (prophylaxis); (2) calcineurin inhibitor; (3) an antiproliferative agent and (4) a corticosteroid.
Triple therapy: Immune suppression regimen with three immunosuppressant, usually a calcineurin inhibitor, an antiproliferative agent plus a corticosteroid.
Dual therapy: Usually a calcineurin inhibitor or an antiproliferative agent plus a corticosteroid.
Monotherapy: Usually a calcineurin inhibitor.
_
The 2 types of induction strategies used to avoid early acute rejection are (1) antibody-based therapy and (2) aggressive early immunosuppression.
- Antibody-based therapy: This therapy uses monoclonal (e.g., muromonab-CD3) or polyclonal antibodies or anti-CD25 antibodies (e.g., basiliximab, daclizumab) and is administered in the early posttransplant period (up to 8 wk). Antibody-based therapy allows for avoidance or dose reduction of calcineurin inhibitors, possibly reducing the risk of nephrotoxicity. All agents are effective for preventing acute rejections, although the anti-CD25 antibodies may require concurrent administration of calcineurin inhibitors. The adverse effect profile of the polyclonal and monoclonal antibodies limits their use in some patients. Patients at highest risk of rejection may receive rabbit antithymocyte globulin (Thymoglobulin).
- Aggressive early immunosuppression: This therapy uses maintenance drugs at higher doses to achieve the strongest immunosuppressive effect soon after transplantation. Approximately 50% of patients do not receive antibody therapy at the time of transplantation. The highest doses of calcineurin inhibitors place patients at increased risk of nephrotoxicity and may not be the best strategy for patients at the highest risk for rejection.
_
Immunosuppression is required for as long as the graft functions; if it is stopped, then rejection occurs and the graft is lost. However, the intensity of immunosuppression is not constant. High levels of immunosuppression are required soon after transplant, but thereafter doses can be reduced to a lower maintenance level. Immunosuppression in that initial period after transplantation is often enhanced by the use of a biological agent, such as a monoclonal or polyclonal antibody, many of which may be started intraoperatively or given immediately before surgery. Historically, anti-lymphocyte globulin, produced by inoculating horses or rabbits with human thymocytes and lymphocytes, was used, but this has been largely supervened by monoclonal antibodies that target specific lymphocyte subsets. One such example is basiliximab, a chimeric monoclonal antibody to the CD25 antigen on the alpha chain of the interleukin 2 receptor, which is only expressed on activated T cells. Basiliximab therefore targets only activated T cells, and in the context of transplantation, these are the ones involved in allorecognition and initiation of an immune response. It has been shown to significantly reduce the incidence of graft rejection, although it is unclear whether it affects long-term survival. Alemtuzumab is another monoclonal antibody that is increasingly being used, and acts by depleting circulating T and B cells. Like the polyclonal anti-lymphocyte globulins, the first dose of alemtuzumab is associated with massive cell lysis and release of cytokines that can cause dramatic haemodynamic instability, an important consideration if administration occurs in the perioperative period. This can be reduced by prior administration of steroids and an antihistamine.
_
Maintenance immunosuppression is the key to prevention of acute and chronic rejections throughout the life of the graft. Maintenance immunosuppressive therapies include small molecule drugs (calcineurin inhibitors and antiproliferatives), fusion proteins and glucorticorticoids. There is also special agents include intravenous immunoglobulin, rituximab, leflunomide, eculizimab and bortezomib.
_
Immunosuppressive regimens:
Immunosuppression is normally given as a combination of agents with different sites of action and different side-effect profiles, following similar principles to antimicrobial and anti-neoplastic chemotherapy. The most common regimen used today in kidney transplantation is a CD25 monoclonal antibody such as basiliximab, followed by a combination of tacrolimus, mycophenolate, and steroids. The regimen will vary according to the perceived immunosuppressive challenge that the transplant poses, with more powerful immunosuppression being used where the risk of rejection is perceived to be highest. Similarly different organs and different diseases require different protocols.
_
Rejection treatment:
Acute:
The 3 agents used to treat acute rejection are (1) steroids, (2) antithymocyte globulin, and (3) muromonab-CD3.
- Steroids: These agents are the mainstay of therapy for acute rejection episodes, preventing release of IL-1 by macrophages and blocking synthesis of IL-2 by helper T cells. Steroids also have anti-inflammatory properties. The typical dosage is 3-5 mg/kg/d for 3-5 days, which is then tapered to a maintenance dose. Steroids reverse 60-75% of rejection episodes.
- Antithymocyte globulin: This agent binds all circulating T and B lymphocytes, which are then lysed or phagocytosed by the reticuloendothelial system. Antithymocyte globulin has efficacy similar to that of muromonab-CD3. It is reserved for steroid-resistant acute rejection secondary to cost, toxicity, and the development of drug antibodies.
- Muromonab-CD3: This agent displaces the T3 molecule from antigen receptors, captures all mature T cells, and prevents alloantigen recognition. The reversal rate of first acute rejection episodes is 94%. Muromonab-CD3 is sometimes used as the first-line agent for severe vascular rejections. The development of human antimurine antibodies allows for the reappearance of CD3 T cells, which may decrease the efficacy of muromonab-CD3 and necessitate higher doses (increasing risk of infection). A second course of muromonab-CD3 may be given for recurrent rejection, although repeat treatment may be associated with complications from the development of antimouse antibodies. The success rate in recurrent episodes is approximately 40-50%.
Chronic:
Unless inadequate immunosuppression is the cause of rejection, changes in immunosuppressive therapy are generally not effective in reversing chronic rejection. The addition of sirolimus to mycophenolate mofetil is currently being studied to determine efficacy. Long-term data on transplanted patients treated with sirolimus demonstrated a chronic rejection rate of 14%, which is much lower than rates traditionally reported in cyclosporine-based regimens.
Control of blood pressure, treatment of hyperlipidemia, and management of diabetes are the current mainstays of treatment for graft preservation.
_
Length of treatment
Although induction of tolerance may allow withdrawal of immunosuppression in the future, at this time, immunosuppressive medications appear to be necessary for the life of the transplanted organ. Episodes of acute cellular rejection have occurred after the cessation of medication even 20 years after transplantation. For patients with stable graft function, individual components of the treatment regimen may be gradually diminished or completely discontinued; however, in most patients, some degree of immunosuppression must be continued. Some patients with severe resistant infections or malignancy related to immunosuppressants require the discontinuation of these medicines.
____
Treatment of antibody-mediated rejection (AMR):
Organ transplantation represents the preferred treatment option for many patients in terminal organ failure. The half-life of transplanted organs, however, is still far from being satisfactory with the vast majority of the organs failing within the first two decades following transplantation. At this stage, it has become apparent that rejection (prevalently mediated by humoral events) remains the primary cause of graft loss after the first year. In this light, studies are underway to better comprehend the immune events underlying graft rejection and novel immunosuppressive strategies are being explored. Antibodies formed in the recipients against the transplanted organ, play a major role in the graft rejection. Thus these antibodies should be removed from the recipients circulation as far as possible. Although the current diagnosis of AMR requires the concomitant presence of DSA, C4d, and histopathological evidence of AMR, treatment may be initiated in circumstances where the above criteria may not be fulfilled in entirety. A number of treatment modalities have been employed for the treatment of AMR as characterized below.
- Antibody removal/neutralization: plasmapheresis, immunoadsorption, intravenous immunoglobulin, and splenectomy.
- Anti B-Cell therapies: Mycophenolate mofetil, Rituximab, IVIG (intravenous immunoglobin), and splenectomy.
- Antiplasma cell therapy: Bortezomib.
- Anti-T-cell therapies: T-cell depleting agents such as Antithymocyte globulin (ATG).
- Conversion to tacrolimus-based regimens.
- Terminal-complement pathway inhibitor: Eculizumab.
IVIG therapy reduces HLA sensitivity by adding helpful antibodies to the patient’s bloodstream. This lowers the level of HLA antibodies and blocks their ability to attack a transplanted organ. IVIG therapy can be used successfully in both adults and children seeking kidney transplants. Unlike many anti-rejection therapies, IVIG does not suppress the entire immune system, but actually boosts the patient’s protection against infection. The presence of a vast array of therapeutic modalities signifies the ineffectiveness of one drug or one particular combination therapy to reverse or treat AMR successfully in all scenarios. All of these treatments have been used in different combinations by different groups without a good control arm, resulting in poor evidence to argue for the superiority of one treatment regimen. These treatment modalities are also used for pretransplantation desensitization protocols to abrogate positive crossmatch in highly sensitized patients.
___
Role of irradiation:
Irradiation to prevent transfusion-associated graft versus-host disease (TA-GVHD) is not recommended on a routine basis for all cases.
Role of leuco-reduction:
Sensitization to HLA antigens can occur even after the use of leucocyte-reduced blood products. Thus the use of these leuco-reduced products must be restricted for prospective renal and heart transplant patients. Although exact role is unknown, it has been shown that leuco-reduction of red cell products are associated with less complications as compared to leucocyte containing transfusions. Cellular blood components used in the pre-, peri- and postoperative setting must be leucocyte reduced to reduce HLA immunization, CMV transmission and prevent post-perfusion complications after liver and cardiac surgery.
__
Toward Individualized Therapy:
A therapeutic development much discussed by the transplant community is a move to more individualized immunosuppression. The way doctors currently individualize immunosuppression is still far behind how some cancer therapies are increasingly being used (for example Herceptin for HER+ breast cancer). In transplantation doctors individualize therapy by clinical history and simple lab tests. They consider the age of the patient, the ethnicity of the patient, the type of donor the patient is getting, the human leukocyte antigens (HLA) match, the level of antibodies and whether there are donor-specific antibodies and we select and individualize immunosuppression on that basis. They then choose depleting vs. non-depleting biologics and the type of maintenance immunosuppression. But they still have not achieved individualization based either on genetic markers or molecular biomarkers. The biomarkers to enable such an individualized approach have not yet been identified or validated in their field.
_
Infection and malignancy issues:
An increasingly recognized problem associated with immunosuppression is BK virus nephropathy. This virus, a member of the human papovavirus family, lives in the human genitourinary tract and replicates in some patients who are immunosuppressed, leading to allograft dysfunction. While antiviral agents such as cidofovir and leflunomide are active against the BK virus, the mainstay of therapy is a reduction in immunosuppression. Opportunistic infections remain an important risk to the immunocompromised patient despite the use of prophylactic measures. Exposure to viruses such as Epstein-Barr virus (EBV), cytomegalovirus (CMV), herpes simplex virus, and human papillomavirus place the donor at risk for infection and, potentially, later malignancy. Posttransplant lymphoproliferative disease (PTLD) is a growing concern in the transplant population. Most of these are of B-cell origin and linked to EBV infections. Patients present with constitutional symptoms such as night sweats, fevers, and weight loss. An acute rise in creatinine levels, similar to acute allograft rejection, may also be seen. Risk factors for PTLD include primary EBV infection; the use of cyclosporine, tacrolimus, and MMF; and an exposure to antithymocyte globulin (ATG) or OKT3. Treatment options include reduction or discontinuation of immunosuppression with an increase in prednisone to reduce rejection risk.
______
______
Preventing Transplant Rejection without Drugs:
The ability to induce tolerance to a transplanted organ, allowing it to thrive in the body without requiring these life-long immunosuppressant, would signify a dramatic improvement in quality of life for patients undergoing organ transplantation. For many in the field, induction is considered the “holy grail.”
_
A 2002 study:
Preventing donor organ rejection in kidney transplant recipients without a lifelong course of immunosuppressive drugs may become a possibility. Researchers at Stanford University Medical Center presented their findings to the American Transplant Congress. The research results are from four patients who had kidney transplants between 12 and 18 months ago. After a kidney was transplanted in each patient, the research team gave that person immunosuppressive drugs, cyclosporine and prednisone, to prevent organ rejection. After transplantation, each kidney recipient received multiple small doses of radiation targeted to the immune system combined with a drug to reduce the number of cells capable of an immune attack. The team then injected blood stem cells from the kidney donor into each recipient. The stem cells made their way to the recipient’s bone marrow, where they produced new blood and immune cells that mixed with the existing blood, allowing the recipient’s immune cells to recognize the donated organ as its own. Each patient was then weaned away from the immunosuppressive drugs.
A 2008 study:
Three independent research teams have successfully performed organ transplantations that do not require the recipient to face a lifetime of immunosuppressant drugs to prevent rejection. Instead, the new techniques prevent rejection by training the immune system to recognize the new organ as its own. The three studies, published in the New England Journal of Medicine, are preliminary and involve only a few patients. But if the techniques can be reproduced in a larger population, they could eliminate one of the most enduring scars of the operation: the need to continue taking sometimes-dangerous immunosuppressant drugs. Blood stem cells are made by bone marrow and give rise to white blood cells, including the B cells that produce antibodies, and T cells that are important in distinguishing host from donor. Researchers found that transplanting these cells into the host created a hybrid immune system. The transplanted organ was no longer recognized as foreign; it was partly ‘self’. Bone-marrow transplantation carries its own risk, but the benefits may outweigh that. The short-term potential risks have to be put up against the long-term risks and the side effects and costs of the drugs. All three of these studies illustrate an emerging understanding of how the immune system can be trained to tolerate foreign cells.
_
![]()
_
Concurrent Bone marrow and Kidney transplant:
To achieve results, researcher first administered drugs known as a “conditioning regimen” to reduce both the immune function and the numbers of the patients’ own bone marrow cells. Next, they performed bone marrow and kidney transplants from living unrelated donors. A short course of immunosuppressant medications was administered immediately after transplantation, and then tapered down and stopped altogether. It was remarkable that tolerance was successful even when the donor’s most potent transplantation antigens were mismatched to the recipient’s. Most bone marrow transplants normally require a match between the donor’s and recipient’s human leukocyte antigen (HLA) system, part of the immune system which encodes the most potent antigens. Performing bone marrow transplants across the HLA barrier usually results in serious, systemic rejection known as graft versus host disease (GVHD). Using immunosuppressant protocol however they achieved significant success without GVHD even across HLA barriers. Most people think of bone marrow transplants as a treatment for people with blood diseases like leukemia or aplastic anemia. But in studies of both patients and animals receiving donor bone marrow cells along with a new kidney, researchers have shown that marrow can influence the recipient’s immune cells to induce tolerance.
Dr. Griesemer explains how the multistep process works with kidney transplants in animals: A week or two before the transplant, the recipient gets treatment meant to deplete a portion of its bone marrow “to make space for the donor cells to engraft,” he says. The recipient is also infused with antibodies that attack and deplete T-cells and B-cells, which normally drive the body’s immune response. Then, on the day the new kidney is transplanted, stem cells from the donor’s bone marrow are extracted and infused into the recipient. The new bone marrow cells appear to dampen immune response to the new organ. “The new bone marrow,” says Dr. Griesemer, “prevents the development of new immune cells that ordinarily would respond to and reject the organ.” Most patients never come off immunosuppressant drugs. But the first patient to receive this treatment at Massachusetts General has survived for almost 15 years, 14 of those without immunosuppressant medication. Six other of Dr. Sykes’ patients also accepted their kidneys for more than five years without immunosuppressant drugs, although three eventually returned to a low level of medication. All of these patients still have their original donor kidney. To that end, the researchers have again been working with bone marrow to try to induce immune tolerance that would allow organs from one species to another to be accepted. The animal research is moving us quickly toward xenotransplantation.
_____
_____
Gene therapy in organ transplantation:
One major complication facing organ transplant recipients is the requirement for life-long systemic immunosuppression to prevent rejection, which is associated with an increased incidence of malignancy and susceptibility to opportunistic infections. Gene therapy has the potential to eliminate problems associated with immunosuppression by allowing the production of immunomodulatory proteins in the donor grafts resulting in local rather than systemic immunosuppression. Alternatively, gene therapy approaches could eliminate the requirement for general immunosuppression by allowing the induction of donor-specific tolerance. Gene therapy interventions may also be able to prevent graft damage owing to nonimmune-mediated graft loss or injury and prevent chronic rejection.
Progress:
- Gene therapy-mediated CD28/B7 costimulatory blockade can prolong graft survival, but results in nonspecific immunosuppression.
- Gene therapy-mediated CD40/CD154 costimulatory blockade can prevent acute allograft rejection, but does not prevent chronic alloreactivity.
- Hyporesponsiveness to virally encoded MHC genes has been induced in both rodent and large animal models.
- Induction of stable long-term T-cell tolerance to MHC class I antigens through central deletion of alloreactive T cells following induction of molecular chimerism.
- Evidence for induction of T regulatory cells that can prevent allograft rejection in gene therapy models.
- Induction of B-cell tolerance by molecular chimerism.
- Induction of tolerance in sensitized recipients.
- Gene therapy-mediated cytokine production, or immune deviation, prolongs graft survival, but does not prevent rejection.
- Transduction of dendritic cells with genes encoding immunomodulatory proteins can moderately prolong graft survival.
- Improved graft survival through antiapoptotic and antiproliferative gene therapy.
_
Transplant genetics and genomics a 2017 study:
Ever since the discovery of the major histocompatibility complex, scientific and clinical understanding in the field of transplantation has been advanced through genetic and genomic studies. Candidate-gene approaches and recent genome-wide association studies (GWAS) have enabled a deeper understanding of the complex interplay of the donor recipient interactions that lead to transplant tolerance or rejection. Genetic analysis in transplantation, when linked to demographic and clinical outcomes, has the potential to drive personalized medicine by enabling individualized risk stratification and immunosuppression through the identification of variants associated with immune-mediated complications, post-transplant disease or alterations in drug-metabolizing genes.
______
______
Nanoparticles used to stop a body rejecting organ transplants a 2017 study:
A team from Yale has now developed an entirely new way of reducing organ transplant rejection by “hiding” the donated organ using targeted nanoparticles. One of the most potent form of immune cells responsible for the body rejecting a transplanted organ is activated by proteins known as human leukocyte antigens (HLAs). These proteins are found on the surface of endothelial cells, which line an organ’s blood vessels. Previous research has shown that small interfering RNA (siRNA) can stifle the expression of these HLAs, lowering the chances of the body rejecting the new organ, but up until now there have been a couple of problems with this form of treatment. General administration of siRNA can negatively affect healthy organs in other parts of the body, and the effects of siRNA tend to only last a few days while a new organ needs several weeks to settle into the body. The novel drug delivery system developed by the team at Yale uses polymer-based nanoparticles to send the siRNA to the desired graft locations and then slowly release the siRNA over several weeks. In the study the team transplanted a small part of a human artery loaded with these siRNA nanoparticles into a mouse inoculated with human T-cells. The results were significantly positive, notably silencing the expression of HLA proteins for up to six weeks. The study also showed no damage to other organs meaning the delivery mechanism was successfully localized. The team is now moving the research focus to kidney transplants, the most common type of organ transplant. A system known as normothermic machine perfusion, developed at Cambridge University, looks to be the best way to deliver these nanoparticles to a donated organ before transplantation. The process involves pumping oxygenated red blood cells through an organ after it is removed from a deceased donor in order to repair any damage. The plan is to add the new nanoparticles to the red blood cells during this process in the hope it will deliver the siRNA to the organ’s endothelial cells prior to implantation in the new patient. If successful, this could significantly reduce the rate of organ rejection in the recipient.
_____
_____
Local immunosuppression:
Systemic immunosuppression frequently results in well-known, but unavoidable, side effects. Conversely, the phenomenon of transplant rejection has been recognized as a local cellular event, with extreme variability noted in rejection even between adjacent cells. Effective local immunosuppression by controlled-release drug delivery systems, such as polymer or biodegradable matrices, might be able to minimize immunosuppressive problems by delivering agents directly to the affected target cells, and optimal drug activity could be achieved with less systemic side effects. The existence of local immune privilege at some specialized tissues, such as the eye, CNS, or pregnant uterus, supports the feasibility of localized immunomodulation.
_
Site-Specific Immunosuppression in Vascularized Composite Allotransplantation: Prospects and Potential, a 2013 study:
Skin is the most immunogenic component of a vascularized composite allograft (VCA) and is the primary trigger and target of rejection. The skin is directly accessible for visual monitoring of acute rejection (AR) and for directed biopsy, timely therapeutic intervention, and management of AR. Logically, antirejection drugs, biologics, or other agents delivered locally to the VCA may reduce the need for systemic immunosuppression with its adverse effects. Topical FK 506 (tacrolimus) and steroids have been used in clinical VCA as an adjunct to systemic therapy with unclear beneficial effects. However, there are no commercially available topical formulations for other widely used systemic immunosuppressive drugs such as mycophenolic acid, sirolimus, and everolimus.
_
Inhaled immunosuppression with tacrolimus (TAC) is a novel strategy after lung transplantation. Rat experiments showed that TAC can be delivered easily and effectively into the lungs without causing airway toxicity, decreases inflammatory cytokine production, and inhibits NF-kB activation. Recent data indicates that local immunosuppression at the site of transplanted graft (rat liver and kidney transplantation) will increase graft survival and reduce the toxicity of immunosuppressive agents in other organs. However, current methods of local immunosuppression have several limitations, which seriously hamper their clinical use.
______
_____
Natural Compounds that Target Pro-inflammatory Cytokines involved in Transplant Immunology:
- Curcumin
Studies of curcumin, a principle component of the Indian spice turmeric, have identified it as a potent anti-inflammatory agent (Sikora, 2010). In particular, numerous studies have revealed the ability of curcumin to target several cytokines involved in transplant rejection, including IL-1, IL-2, IL-6, IL-21 and TNFα (Jurrmann, 2005; Kim, 2009; Zhang, 2010; Xie, 2009). An experimental study found that curcumin, in combination with cyclosporine, significantly improved survival time in animals that received a cardiac transplant from donors with incompatible genotypes. Animals treated with curcumin and cyclosporine survived for an average of 28.5 – 35.6 days after receiving a transplant, compared to untreated animals, which survived an average of only 9.1 days. The effect of the combination of curcumin and cyclosporine was greater than the effect of either one alone. The authors concluded that curcumin is efficacious as a novel adjuvant for immune system modulation both in vivo and in vitro (Chueh, 2003). To more closely examine the immunomodulatory effects of the spice, researchers analyzed the effects of curcumin on lymphocytes of renal transplant patients who were experiencing transplant rejection. They found that the use of curcumin dose-dependently decreased interferon-alpha (an inflammatory cytokine) induction in cultures from patients experiencing acute rejection (38.3%-18.3%) and those experiencing chronic rejection (40.6%-12.9%), when compared with corresponding untreated cultures. Furthermore, the team also noted that curcumin was able to inhibit activation of nuclear factor kappa β (NF-kappa β), an inflammatory transcription factor, and inhibit proliferation of T-cells, having a synergistic effect when combined with cyclosporine. The researchers concluded that curcumin was a pharmacologically safe adjuvant to be used with cyclosporine, and can effectively suppress inflammatory cytokine induction after renal transplant (Bharti, 2010).
- Omega-3 fatty acids
Omega-3 fatty acids, also known for their potent anti-inflammatory properties, are capable of suppressing the inflammatory cytokines IL-1, IL-2, IL-6, IL-15 and TNFα (Cooper, 1993; Manzoni, 2009; Wang, 2008; Muurling, 2003). Researchers examined the endothelial function, as measured by endothelium-dependent vasodilation, of seven cardiac transplant patients who consumed 5,000 mg of EPA plus DHA daily for three weeks and compared the results to those of seven cardiac transplant control patients who did not receive fish oil. The researchers found that endothelium-dependent vasodilation was significantly improved in the fish oil group (+14% to +15%), while it worsened in the control group over the study period (-1% to -9%) (Fleischhauer, 1993). In another study, researchers examined the effect of six grams of fish oil taken daily for one month in 40 cyclosporine treated patients who had received a transplanted kidney. It was found that fish oil-treated patients showed a significantly better recovery of renal function after a histologically confirmed rejection episode compared to control. The researchers went on to conclude that “dietary supplements with fish oil favorably influence renal function in the recovery phase following a rejection episode in cyclosporine-treated renal transplant recipients” (Homan van der Hide, 1992). To evaluate the perioperative safety of fish oil in a transplant population, researchers evaluated hemodynamic, biochemistry and hematological parameters in kidney recipients who received intravenous fish oil for five days postoperatively. The researchers concluded that “administration of [omega-3 fatty acids] is safe in organ donors and in kidney recipients” (Singer, 2004).
- Resveratrol
Studies conducted on resveratrol provide strong evidence that suggests it can help quell the cytokine storm and prolong the survival of transplanted tissue. Resveratrol has been shown to attenuate the action of the cytokines IL-1β, IL-2, IL-6 and TNFα (Shakibaei, 2007; Yu 2005; Wung, 2005; Leiro, 2010). Resveratrol, at a dose equivalent to 967 mg for a 60 kg human, was shown to significantly increase survival time of animals that received a genetically incompatible liver transplant. Furthermore, resveratrol also reduced levels of cytotoxic T-cells (Wu, 2006). In a skin graft model, used to study transplant rejection, rats supplemented with relatively small doses of resveratrol, equivalent to approximately 5 mg for a 60 kg human, had notable prolongation of the time period before their skin grafts were rejected. Only ~20% of the allografts in the control group survived greater than nine days post-operation, compared to 100% of the grafts in the group receiving resveratrol. The researchers noted that resveratrol significantly reduced infiltration of T-cells and necrosis in graft tissue (Hsieh, 2007).
- Green and Black Tea Polyphenols
Compounds in green and black tea have been identified as particularly powerful anti-inflammatory agents (de Mejia EG, 2009). Studies have shown that components of tea are potent inhibitors of IL-1β, Il-2, IL-6 and TNFα (Wheeler, 2004; Wu, 2009; Hosokawa, 2010; Yuan, 2006). Cardiovascular health is a major concern for transplant recipients, especially because cyclosporine, an immunosuppressive drug widely used after organ transplantation, is known to impair endothelial function (Morris, 2000). Black tea consumption was shown to dramatically improve endothelial function, as measured by flow-mediated vasodilation and brachial artery diameter, in a study of renal transplant patients aged 25 – 50 years. The researchers went on to conclude that “based on our study, short-term consumption of black tea may improve endothelial function and endothelium-dependent arterial vasodilation in renal transplant recipients” (Ardalan, 2007).
- Quercetin
The flavonoid quercetin is found in significant quantities in apples, onions, grapes and citrus fruits. Quercetin is known to modulate the action of several inflammatory cytokines that are of particular concern to transplant recipients, including IL-1β, IL-2, IL-6, IL-15 and TNFα (Ying, 2009; Yu, 2008; Liu, 2005; Karlsen, 2010; Ruiz, 2007). Quercetin, in combination with vitamin E, has also been shown in vitro to combat the hepatotoxic effects of cyclosporine. Researchers found that the combination attenuated cyclosporine induced oxidative stress by restoring the activity of the antioxidative enzymes glutathione peroxidase and catalase. They concluded that “our data demonstrates that vitamin E and quercetin play a protective role against the imbalance elicited by cyclosporine between the production of free radicals and antioxidant defence systems, and suggests that a combination of these two antioxidants may find clinical application where cellular damage is a consequence of reactive oxygen species” (Mostafavi-Pour, 2008). Considering the cytokine suppressive effects of quercetin, a team of researchers evaluated the impact of quercetin on the proliferation of T-cells. The team found that quercetin significantly inhibited T-cell proliferation, suggesting that it may be effective in reducing transplant rejection. They concluded “these results suggest the potential use of these select phytochemicals for treating autoimmune and transplant patients…” (Hushmendy, 2009).
- Vitamin D
Published studies in recent years have revealed an astonishing number of benefits attributable to vitamin D. Among these benefits, modulating the activity of multiple inflammatory cytokines is especially important in the context of organ transplantation. Researchers recently discovered that vitamin D was able to prevent a cyclosporine mediated increase in the inflammatory cytokines IL-1β, IL-6 and TNFα in an animal model (Spolidorio, 2010).Vitamin D, in combination with cyclosporine, significantly reduced production of IL-2 and the proliferation of T-cells, and vastly prolonged allograft survival in an animal model of liver transplantation. The authors of this study went on to conclude that vitamin D is effective as an adjunct to immunosuppressive therapy for the prevention and treatment of liver graft rejection (Zhang, 2006). A very important 2009 study shed light on just how critical vitamin D supplementation is for transplant recipients. Researchers examined the relationship between blood levels of the active form of vitamin D (1,25-dihydroxy vitamin D) and one-year mortality rates of heart transplant patients. They found that “one-year mortality was 3.7 per 100 person-years in the tertile with the highest [1,25-dihydroxy vitamin D] concentrations, 13.2 per 100 person-years in the intermediate tertile and 32.1 per 100 person-years in the tertile with the lowest concentrations.” This means that the mortality rate was over eight times higher at one year post-transplant in the group with the lowest one-third blood levels of active vitamin D compared to the group with the highest one-third levels of active vitamin D. The researchers also found that higher blood levels of vitamin D were associated with lower levels of the inflammatory marker C-reactive protein, as well as the cytokine TNFα (Zittermann, 2009).
______
______
Obesity and ODT:
Transplantation in obese individuals:
You could be too obese to have a transplant:
The American Society of Transplantation advises patients to get their weight down before a transplant, to a BMI of 30 or less. This corresponds to less than 203 pounds for a person who is 5-feet 9-inches tall. When you are obese, you may have more health problems after a transplant than someone who weighs less, a review of studies found. Obese people are more likely to have infections at the wound site of a transplanted kidney, and the new organ fails to function more often as well. People who are obese are also at greater risk of developing heart disease after a transplant compared to people who weigh less. Until recently, people labelled as obese were not considered appropriate candidates for renal transplantation. In 2009, the physicians at the University of Illinois Medical Center performed the first robotic kidney transplantation in an obese recipient and have continued to transplant people with Body Mass Index (BMI)’s over 35 using robotic surgery. As of January 2014, over 100 people that would otherwise be turned down because of their weight have successfully been transplanted.
_
Obesity linked to inflammation and organ transplant rejection:
One of the reasons obesity is so dangerous for long-term health is that it produces low-grade, chronic inflammation. This kind of inflammation revs up the immune system, which can aggravate other chronic conditions like asthma, high blood pressure, and digestive disorders. A recent study by researchers at the University of Chicago suggests that obesity increases the risk of organ transplant rejection as well. It’s a troublesome finding when more and more transplant recipients are likely to be overweight, putting them at greater risk in an already precarious state of health. In obese individuals, adipocytes, or fat cells, become enlarged and undergo stress. These adipocytes produce cytokines, proteins that give signals to other cells, which rev up the immune system. These cytokines could be triggering the stronger T-cell response to the transplanted organ. Obese individuals also tend to have higher levels of cholesterol, lipids, and glucose circulating in the blood, all of which could enhance the immune response against the transplant. Another intriguing possibility is the role played by the microbiota, or the millions of bacteria and other microorganisms living in the digestive tract and other body surfaces. Previous research has shown that obesity can change the composition and behavior of these microbiota—it’s possible that these changes affect how the microbiota interact with immune cells that recognize the antigens introduced by the organ transplant. This could in turn affect the level of tolerance the immune system has for these antigens, and speed up the rejection process.
_
Adiponectin and heart transplant rejection:
Adiponectin is negatively associated with body mass index, waist circumference, percent fat mass, triglycerides, and insulin resistance. It is well known that adiponectin levels are lower in obese patients. In heart transplant recipients, plasma adiponectin levels were found to be normal or higher, probably due to renal failure (Ambrosi et al., 2009). However, higher plasma adiponectin levels may predict better outcome among recipients of heart transplant, as adiponectin inhibited allograft rejection in a murine cardiac transplantation model (Okamoto et al., 2009). These data suggested that adiponectin reduces allograft rejection by blocking lymphocyte proliferation and recruitment, therefore providing beneficial effects in inhibiting alloimmune responses. This pathway may represent a new therapeutic target for allograft rejection after heart transplantation.
_______
_______
Pregnancy and ODT:
_
Brain death and pregnancy:
Pregnancy can be prolonged after brain death. It is then possible to deliver the baby by means of caesarian section. Cadavers have been reported to support a fetus for a period of 107 days. Since 1981 there have been 22 recorded instances of keeping a mother declared brain dead in a beating heart cadaver state until the baby is delivered. After delivering the baby, some cadavers have subsequently become organ donors.
_
Pregnancy and Transplantation:
End-stage organ disease disrupts normal gonadal function; consequently, pregnancies in patients with end-stage disease are relatively uncommon. Fertility is improved within months after the successful replacement of an infirmed organ; therefore, it is not surprising that increasing numbers of pregnancies are reported in patients with transplanted kidneys, liver, heart, lungs, and small bowel and even in those with multiple organ transplants. Optimal contraception is important to initiate before transplantation in women of childbearing age. Contraception should be used before transplantation, because there have been several reports of women who were pregnant in the peritransplantation period. The peritransplantation period is not the optimal time for pregnancy because this is a time of highest use of potentially fetotoxic or teratogenic medications and a time when optimization of immunosuppression is essential. Compared to the general population, a female transplant recipient has about a three times greater chance of having a baby who is premature (born before 37 weeks) or low birth weight (weighing less than about five and one half pounds). Current data suggest that protocols involving cyclosporine, azathioprine, and steroids are associated with low rates of birth defects, although patients are treated with high-risk pregnancy strategies. Preliminary data also suggest the safety of tacrolimus and Mycophenolate mofetil in animal data and some early human studies show adverse effects on fetal development. Presently, few data exist regarding sirolimus and pregnancy. Several recent studies have indicated that the benefits of breastfeeding outweigh the potential risks. Studies have shown that only a tiny amount of these medications is passed on to the infant through breast milk.
_______
_______
Age and ODT:
The analysis of influence of donor age on outcome in 1991 showed that satisfactory graft survival can be achieved using older donors and that age in itself should not be a barrier to organ donation, providing that organ function is normal and that specific disease of the organ is absent.
_
The number of people over 65 years of age seeking and receiving organ transplants is growing. Presently, the average age of those receiving kidney transplants is approximately 50 years. A similar trend is observed with other organ transplants: approximately 50% of patients who received cardiac transplants between 2002 and 2010 were over 50 years of age, and over 20% were older than 60 years. Along these lines, clinical studies have demonstrated that solid-organ transplantation is an effective treatment for selected older patients. However, older transplant recipients succumb to more infections and are more susceptible to post-transplant malignancies. Most clinical studies in solid-organ transplantation (including heart, kidney, and lung) indicate that increased recipient age (age range, 50 to >70 years) is associated with a reduced frequency of acute allograft rejection, although acute graft rejection in older transplant recipients may be more severe than in younger recipients. Despite a growing body of evidence on the complex effects of immunosenescence, there have been relatively few studies that have focused on aging and the immune response to organ transplantation. In addition, most therapeutic trials in organ transplantation have not included patients over 65 years of age.
Besides the impact on the recipient’s immune response, aging also affects the donor organ before transplantation. Older organs can exhibit more pronounced immunogenicity, respond differently to stress, and repair less well than younger organs subsequently to transplantation. These limits are due to the deleterious effects of aging on organ function, the vasculature, and alterations of resident immune cells, all of which limit the expansion of the donor pool for patients awaiting organ transplantation.
_
Figure below shows impact of aging on donor organ and recipient immune system during organ transplantation.

Aging increases the immunogenicity of the donor allograft, in part owing to passenger DCs. With aging, the donor graft has less tolerance in response to ischemia/reperfusion injury and likely has a reduced capacity to repair after implantation. Old grafts lead to increased transplant vasculopathy through unknown mechanisms. After transplantation, aging impairs CD8+ T cell responses to reject organ transplants, although CD8+ T cells may also impair immune modulation. CD4+ Th1 T cell responses are reduced but IL-17 production is increased with aging. Decreased Treg output from the thymus may impair transplantation tolerance in aged recipients. The aged B cell pool may enhance T cell alloreactive priming and may pose a barrier to immune modulation.
_
Aging has broad and complex effects on both the immune system and organ function as seen in the figure above. Given the rise in the number of older people receiving organ transplants, how aging impacts both the donor allograft and the recipient immune system is poorly understood in contrast to other areas in the transplant field. Clinically, older organs elicit a more potent immune response that leads to a faster tempo of acute graft rejection with increased vasculopathy. Older transplant recipients exhibit reduced frequency of acute allograft rejection but an increased prevalence of infections and malignancies due to the consequences of immunosenescence. Functional alterations in both recipient T and B cell populations may slow the tempo of acute allograft rejection in older recipients, but these populations of immune cells may also hinder the induction of transplant tolerance. Many unanswered questions remain, including how aging impacts transplant vasculopathy, how it affects the innate immune system to alter IRI, and how it influences transplantation tolerance. These are just some areas that need to be investigated in the future. Increasing our fundamental knowledge of how aging is involved in the immune response to organ transplantation can ultimately lead to age-specific therapies to improve health outcomes for older transplant recipients.
______
______
Impact of gender on organ transplantation:
The gender of donors and recipients is involved in the entire process, including organ donation and transplant surgery. In general, women seem to have more self-sacrifice and sense of responsibility than men. As a consequence, it has been observed that women are more predisposed to donate their organs. In fact, in cost-free living donation, two thirds of all organs were donated by women. In contrast, women are less disposed than males to accept transplant surgery. Despite comprising 35 % of transplants, the number of female transplant recipients continued to decline. Several factors have been suggested to explain these differences. Nowadays, women and men present different social, economic, and cultural roles, and a disparity of knowledge may exist. In fact, women were considered to have less information about transplantation diagnosis and therapy. However, besides these psychosocial aspects, another important factor should be considered to explain the above reported gender bias: men have a higher incidence of end-stage diseases that necessitate a transplant and are more inclined to hypertension or ischemic heart disease, leading to their inappropriateness as donors. Regarding graft outcome, male recipients have been observed to have a worse prognosis than females and this could be partially explained by the observation that women have better immunosuppressant compliance than men; they undergo follow-up visits and habit change and show more concern with regard to protecting graft function.
_
Impact of sex on organ transplantation:
Several clinical studies have connected the use of female donor organs as a risk factor for death and rejection. In renal transplantation, female donor kidneys have a worse 5-year survival and this observation could be explained by the lower number of nephrons in the female kidney in comparison to men. In addition, animal experiments suggested that kidneys of females express more HLA antigens and are more antigenic. Moreover, male grafts are less susceptible to nephrotoxic effects of some immunosuppressants than female grafts. Long-term retrospective studies in renal transplants revealed that male recipients undergo a worse survival in comparison to females. It can be hypothesized that protection afforded by hormones in women could result in their better long-term prognosis. Estradiol can in fact improve graft function, preserve graft architecture, and diminish cellular infiltration, including mononuclear cell infiltration.
_
The impact of sex mismatch on transplant outcome still remains a matter of debate:
Male tissues contain XY chromosomes. When male tissue with XY is grafted to female (XX), females don’t contain genes on Y chromosome. The grafts may not be accepted. However grafts done from female to male are accepted. This Phenomenon is called as unilateral sex linked Histocompatibility is known as EICHWALD SILMSER effect.
_
Minor H antigens are now known to be peptides derived from polymorphic proteins that are presented by the MHC molecules on the graft. MHC class I molecules bind and present a selection of peptides derived from proteins made in the cell, and if polymorphisms in these proteins mean that different peptides are produced in different members of a species, these can be recognized as minor H antigens. One set of proteins that induce minor H responses is encoded on the male-specific Y chromosome. Responses induced by these proteins are known collectively as H-Y. As these Y chromosome-specific genes are not expressed in females, female anti-male minor H responses occur; however, male anti-female responses are not seen, because both males and females express X-chromosome genes. One H-Y antigen has been identified in mice and humans as peptides from a protein encoded by the Y-chromosome gene Smcy. An X-chromosome homologue of Smcy, called Smcx, does not contain these peptide sequences, which are therefore expressed uniquely in males. Studies on renal transplantation observed that male donor to female recipient combination is an independent risk factor for poor graft survival and the significantly higher percentage of H-Y antibody production in the male donor-female recipient population could play a role in this phenomenon.
_
In contrast with these studies, other studies reported that female donor to male recipient grafts seems to have a worst prognosis in particular for liver and heart transplantation. In particular, in a recent single-center retrospective study, Schoening et al., evaluating the effect of sex differences on long-term graft survival after liver transplant, found that female donor-male recipient combination showed the worst graft survival. They suggested that this event could be caused by the reduced female donor “quality” (female donors were significantly older, died significantly more frequently from cerebrovascular causes and less frequent by trauma) and by unfavorable characteristics of male recipients (higher incidence of hepatocellular carcinoma in the male recipient group). Interestingly, in studies carried out in animal models, livers from female rats have been demonstrated to present an increased acidosis during transplant-associated ischemia in comparison with livers from male rats; this sex difference in the liver’s metabolic response to ischemia appeared estrogen-mediated and could have a significant influence on the outcome of transplantation. Since a similar sex-dependent metabolic response has been found also in myocardial function, the possibility that this sexual disparity could influence cardiac transplants cannot be ruled out.
______
______
Disadvantages of ODT:
- Organ donations can lead to other health problems:
Organ donation is major surgery. All surgery comes with risks such as bleeding, infection, blood clots, allergic reactions, or damage to nearby organs and tissues; both for living donor and recipient. Although you will have anaesthesia during the surgery as a living donor, you can have pain while you recover. Pain and discomfort will vary depending on the type of surgery. And you may have visible, lasting scars from surgery. It will take some time for your body to recover from surgery. You might have to miss work until you’re fully healed.
- Not every organ which is donated will be accepted:
Organ rejection is a very real possibility for those who receive a transplant. Even when there is a good match, there is always the chance that the transplant will be rejected. Those who receive a transplant will often be required to take immunosuppressant medications for the rest of their lives to reduce the chances of this issue from occurring.
- Complications (vide infra):
Several studies have also shown that patients who have received an organ are at a high risk of developing Type 2 diabetes, though doctors are not exactly sure why. In a review of organ transplant recipients, 10% of them have gone on to develop diabetes at some point in their lives. General illnesses are more common as well because drugs must be taken to suppress the immune system so the new organ won’t be rejected. Immunosuppression in recipient leads to infection and cancer. A transplanted organ can carry a hidden disease along with it. Before transplant, organs are screened for common infections and diseases. This is to exclude any potentially dangerous contamination. Still, one or two people out of every 100 who receive an organ transplant — up to 560 people in the United States each year — contract a hidden infection or disease along with it, data from the U.S. Centers for Disease Control and Prevention shows. Infectious diseases linked to transplants include viral, bacterial, fungal, and even parasitic illnesses.
- Organ transplants are incredibly expensive:
When you undergo a major organ transplant, you need to consider the cost of both the medical and non-medical aspect.
- Medical costs
-Evaluation and testing prior to the transplant
-Insurance co-payments or deductibles
-Surgery costs (surgeon’s fee, operating room fee)
-Recurrent lab testing fees
-Hospital fees
-Expenses of procuring the organ
-Fees for other professionals: doctors, radiologist, anaesthesiologist
-Anti-rejection medication, which can cost more than £1,000 monthly
-Cost of therapy or rehabilitation
- Non-medical costs
-Transportation costs going to and fro the transplant hospital (for you, your carer and loved ones)
-Board and lodging for your loved ones, especially if the transplant hospital is not near your house
-Communication costs
-Housekeeping or childcare costs, while a spouse acts as the carer
-Lost income
_
In the United States, the cost of a liver transplant is $71,000, plus an additional $25,000 for every 30 days of care pre-transplant. For those who need a heart-lung transplant, the cost is $130,000, with an additional $56,000 for every 30 days of care pre-transplant. For many organ recipients, their total care cost exceeds $1 million, with heart-lung transplant recipients facing a cost of $2.3 million. Part of this cost is due to the wait time to receive an organ transplant. For some organs, the average wait time can be 3-5 years in some regions of the United States. Organ transplants in India are prohibitively expensive. There are very few public hospitals performing transplants. More than 95% of organ transplants especially of organs like livers and hearts are currently performed in the private sector where costs range from Rs 2 to 2.5 million. Even relatively less complex kidney transplants cost Rs 1 million. The costs of tests on the deceased donor and transport – which can run into few hundred thousand if they are airlifted – are often transferred to the recipient. Though there are allocation criteria for organs in all states, structural inequity allows organs donated as a public good going to those who can afford them rather than those who need them the most.
_
- Chances for illegal Business with the Organs:
Despite being illegal in several nations, the illicit trade of the human organs has been widespread globally with rich amounts of money on the line. Most of these rackets have been ousted but some of them are still working. The unstabilized ratio of the required and the available organs is said to be the reason for the responsible for the illegal trade to happen. It has indeed said to have become a pity that due to the rich money that is involved in the business, many people like the prisoners and small children are sometimes kidnapped to trading the organs and thereby forced to donate their organs.
One of the driving forces for illegal organ trafficking and for “transplantation tourism” is the price differences for organs and transplant surgeries in different areas of the world. According to the New England Journal of Medicine, a human kidney can be purchased in Manila for $1000–$2000, but in urban Latin America a kidney may cost more than $10,000. Kidneys in South Africa have sold for as high as $20,000. Price disparities based on donor race are a driving force of attractive organ sales in South Africa, as well as in other parts of the world. In China, a kidney transplant operation runs for around $70,000, liver for $160,000, and heart for $120,000. Although these prices are still unattainable to the poor, compared to the fees of the United States, where a kidney transplant may demand $100,000, a liver $250,000, and a heart $860,000, Chinese prices have made China a major provider of organs and transplantation surgeries to other countries.
___
___
Quality and safety of ODT:
All transplanted human organs carry potential risks to the recipient, either from unsatisfactory organ function or disease transmission from the donor to the recipient, with malignancy and infectious diseases being the most relevant. In the case of living donors, there are also the risks to the donor, both immediate and longer term. Knowledge of these risks is a pre-requisite for consent. However, for some recipients—faced with imminent death without a transplant—even significant risks associated with a specific organ or its donor may be acceptable and better than the alternative of imminent death. From the recipient’s point of view, it is therefore important to approach quality and safety in terms of the risk–benefit balance rather than by attempting to eradicate risk entirely.
In November 2007, the CDC reported the first-ever case of HIV and Hepatitis C being simultaneously transferred through an organ transplant. The donor was a 38-year-old male, considered “high-risk” by donation organizations, and his organs transmitted HIV and Hepatitis C to four organ recipients. Experts say that the reason the diseases did not show up on screening tests is probably because they were contracted within three weeks before the donor’s death, so antibodies would not have existed in high enough numbers to detect. The crisis has caused many to call for more sensitive screening tests, which could pick up antibodies sooner. Currently, the screens cannot pick up on the small number of antibodies produced in HIV infections within the last 90 days or Hepatitis C infections within the last 18–21 days before a donation is made. NAT (nucleic acid testing) is now being done by many organ procurement organizations and is able to detect HIV and Hepatitis C directly within seven to ten days of exposure to the virus.
______
The risks for patients undergoing kidney transplantation:
The kidney failing in the first year–10 out of 100
Bleeding needing blood transfusion –5 out of 100
Problem with the join between the kidney and the bladder –7 out of 100
Blockage of the blood vessels supplying the kidney –2 out of 100
Narrowing of the blood vessels supplying the kidney– 5 out of 100
Wound infection –5 to10 out of 100
Collection of fluid around the kidney –7 to10 out of 100
Blood clots in the legs–1 to 3 out of 100
Acute rejection of the new kidney–15 out of 100
Delayed kidney functioning requiring the need for dialysis –40 out of 100
Risks of acquiring infections or transmissible cancers from the donor– 1 out of 20000
______
Complications that can occur after transplantation include
- Rejection (discussed vide supra)
- Infections
- Cancer
- Atherosclerosis
- Kidney problems
- Gout
- Graft-versus-host disease
- Osteoporosis
_____
Opportunistic Infections and Cancer:
As previously discussed, the immune system’s primary role is to identify and attack anything that is foreign or non-self. The main targets were not intended to be transplanted organs, but rather bacteria, viruses, fungi, and other microorganisms that cause infection. Taking immunosuppression weakens a transplant recipient’s defenses against infection. As a result, transplant recipients are at increased risk to develop not only standard infections that may affect all people but also “opportunistic” infections, infections that only occur in people with compromised immune systems. The changes in the immune system predispose transplant recipients to different infections based on the time relative to their transplant operation.
_
Timetable of infection:
With standardized immunosuppressive regimens, most common infections occur in a relatively predictable pattern depending on the time elapsed since transplantation (Figure below). This is a reflection of changing risk factors over time: surgery/hospitalization, immunosuppression, emergence of latent infections, and community exposures. The pattern of infection changes with alterations in the immunosuppressive regimen, including side effects, viral infections, graft dysfunction, or significant epidemiologic exposures (e.g., travel or food). Risk also depends on exposures via donor organs. Prophylactic antimicrobial agents will delay, but not eliminate, the “normal” appearance of infections. Any reduction in the net state of immunosuppression will reduce risk of infection when prophylaxis is discontinued. The time line represents three overlapping periods of risk: (1) the perioperative period to approximately 30 days after transplantation; (2) the period from 1 to 6–12 months after transplantation (reflecting immunosuppression including “induction” therapies and prophylaxis); and (3) beyond 6–12 months posttransplantation.
_
![]()
Figure above shows timeline of infections following organ transplantation. The pattern of common infections following organ transplantation varies with the net state of immunosuppression and the epidemiology of infectious exposures. Development of disease is delayed, but not eliminated by prophylaxis including vaccinations and antimicrobial agents. Individual risk is modified by events including treatment for graft rejection or malignancy. The time line is used to (1) establish a differential diagnosis for the transplant patient suspected of having infection, (2) identify excess environmental hazards or over‐immunosuppression, and (3) design preventative antimicrobial strategies. Infections occurring at the “wrong” time suggest an excessive epidemiologic hazard or excessive immunosuppression. The prevention of infection is linked to the expected risk of infection.
_
Factors contributing to the “net state of immunosuppression”:
Immunosuppressive Therapy: Type, Temporal Sequence, and Intensity
Prior therapies (Chemotherapy or Antimicrobials)
Mucocutaneous Barrier Integrity (catheters, lines, drains)
Neutropenia, Lymphopenia, Hypogammaglobulinemia (often drug‐induced)
Technical complications (graft injury, fluid collections, and wounds)
Underlying immune defects (e.g. genetic polymorphisms, autoimmune disease)
Metabolic conditions: uremia, malnutrition, diabetes, alcoholism/cirrhosis, advanced age
Viral infection (e.g., herpes viruses, hepatitis B and C, HIV, RSV, influenza)
HIV, human immunodeficiency virus; RSV, respiratory syncytial virus.
_
Before 1980, nearly two-thirds of kidney and liver transplant recipients developed at least one infectious complication in the first year post-transplant that was associated with a mortality rate approaching 50%. Currently, 1-year mortality caused by infection has decreased to less than 5% for renal transplant patients and is down to 10% in liver allograft recipients. Advances in surgical techniques, organ preservation, and improved postoperative care have contributed to more favorable outcome in these patients. Other factors that have positively impacted infection rates in these patients include pretransplant evaluation by infectious disease experts, vaccination, primary antibiotic prophylaxis, improved diagnostics, pre-emptive antibiotic therapy in high risk patients, and effective infection control practices. More selective immunosuppressive agents and more attention to prevention of cytomegalovirus (CMV) infection have been among the most significant changes. Despite these advancements, infection remains a serious life-threatening complication of solid organ transplantation. The risk of infection is directly related to the functional status of the immune system. A complex interplay of factors determines the net state of immunosuppression in solid organ transplant recipients. These factors include the presence of underlying diseases, postoperative metabolic factors, and concurrent infection with immunomodulatory viruses such as CMV, Ebstein-Barr virus (EBV), and HIV. More importantly, the type, dose, and duration of immunosuppressive therapy required to prevent and treat allograft rejection is the critical determinant of immune competence in SOT patients. Donor-derived tuberculosis (TB) is a rare but important complication of solid organ transplantation. When donor-derived TB disease is identified in an organ recipient, other patients who received organs from the same donor should be evaluated and, when indicated, treated for TB infection or disease.
_______
_______
Transplant-Related Malignancies:
Malignancy is a problem that requires careful consideration in the evaluation of organ donors and transplant recipients both before and after transplantation. Utilization of organs from donors with malignancy, allocation of organs to transplant candidates with a history of malignancy, and factors related to development and treatment of recurrent or de novo posttransplant neoplasias serve as referential points from which to raise a number of issues. In addition to fighting infection, the immune system also fights cancer. It is believed that a healthy immune system detects and eliminates abnormal, cancerous cells before they multiply and grow into a tumor. It is well-recognized that transplant recipients are at increased risk for developing several specific types of cancers. The application of immunotherapy, particularly cell therapy, to both infectious disease and neoplasia in the solid organ transplant population is undergoing a period of rapid development.
Neoplasia in the Donor:
Cancer may be transferred from an organ donor to a recipient as a result of occult malignancy in the donated organ or misdiagnosis, in a known situation such as when a small renal cell carcinoma occurs in the donor kidney and undergoes wide excision, in a low-risk situation such as when the donor has a known skin malignancy or carcinoma in situ of the cervix, or when a known cancer was believed to have been cured. In addition, de novo malignancy may arise from either graft parenchymal cells or passenger cells in the graft.
In the past, many types of tumors have been considered absolute contraindications to organ donation. Today, however, 2 tumors — choriocarcinoma (93% transmission, 64% mortality) and melanoma (74% transmission, 60% mortality) — fall into this category. In addition, since lung cancers and sarcomas, particularly high-grade variants, also behave aggressively, procuring organs from donors with these tumors is not recommended.
_
Organ transplant confers a 2- to 4-fold increase in solid organ malignancies and up to a 30-fold increase in lymphoproliferative malignancies compared with the general population. This increased risk seems to be directly related to long-term use of immunosuppression, which can lead to disruptions in normal immune surveillance of malignant cells and also leads to increased risk of oncogenic viral infections, such as Epstein-Barr virus (EBV), human papillomavirus (HPV), and human herpesvirus 8 (HHV8). Another factor is the increasing age of transplant recipients and the presence in these patients of comorbid conditions that increase their cancer risk, such as obesity, alcohol use, and tobacco use.
_
Post-Transplant Lymphoprolipherative Disorder (PTLD):
Post-Transplant Lymphoprolipherative Disorder (PTLD) is an unusual type of cancer that arises exclusively in transplant recipients, as suggested by its name. It is almost always associated with Epstein-Barr virus (EBV), the same virus that causes infectious mononucleosis. PTLD arises when EBV-infected B cells (a subset of lymphocytes) grow and divide in an uncontrolled fashion. As it is fundamentally a result of a compromised immune system, the first line of treatment is simply stopping or substantially reducing immunosuppression. While this approach frequently works, it also risks graft rejection which would then necessitate increased immunosuppression. Recently, a drug that specifically eliminates B cells, the cells infected by EBV, has become available. Today, a common approach is therefore to give this drug, rituximab, in conjunction with less drastic cuts of the immunosuppression drugs. If this approach does not control PTLD, then more conventional chemotherapy drug regimens typically given to treat lymphomas that develop in non-immunosuppressed patients, are used. The majority of PTLD cases can be successfully treated with preservation of the transplanted organ.
Non-Melanoma Skin Cancer (NMSC):
Skin cancers are the most common malignancy in the post-transplant population. The rate of skin cancer in patients who have undergone organ transplantation is 27% at 10 years, reflecting a 25-fold increase in risk relative to the normal population. The risk of squamous cell carcinoma is about 100 times higher after a transplant compared with the general population’s risk. In light of this substantial risk, it is strongly recommended that all transplant recipients minimize sun exposure. Moreover, all transplant recipients should be regularly examined to ensure early diagnosis and expeditious treatment of any skin cancer. There is some evidence to suggest that sirolimus, an immunosuppressant in the class of mTOR inhibitors (see Immunosuppression section) does not increase risk of skin cancers. Therefore, transplant recipients who develop multiple skin cancers can be considered for a switch to a sirolimus-based, calcineurin-inhibitor free immunosuppression regimen. Currently, there is no data to indicate that liver transplant recipients are at increased risk to develop other common cancers such as breast, colon, prostate, or other cancers.
_______
_______
Neurological Complications of Solid Organ Transplantation:
Solid organ transplantation is a significant development in the treatment of chronic kidney, liver, heart and lung diseases. This therapeutic approach has increased patient survival and improved quality of life. New surgical techniques and immunosuppressive drugs have been developed to achieve better outcomes. However, the variety of neurological complications following solid organ transplantation is broad and carries prognostic significance. Patients may have involvement of the central or peripheral nervous system due to multiple causes that can vary depending on time of onset after the surgical procedure, the transplanted organ, and the intensity and type of immunosuppressive therapy. Neurologically important syndromes such as immune reconstitution inflammatory syndrome (IRIS), posterior reversible encephalopathy syndrome (PRES), and posttransplantation lymphoproliferative disorder (PTLD) deserve special mention. Neurological manifestations following solid organ transplantation pose a diagnostic challenge to medical specialists despite extensive investigation. On the other hand, organ transplantation may also improve neurologic function in various disorders with neurologic manifestations such as Wilson disease (liver transplantation), familial amyloidosis with neuropathy (liver transplantation), and diabetic neuropathy (pancreas transplantation).
_
Main neurological complications in solid organ transplant patients.
| Central nervous system infections: | |
| Viral infections (herpes virus family and polyomavirus) | |
| Bacterial infections (Nocardiosis, Listeria monocytogenes and Mycobacterium tuberculosis) | |
| Fungal infections (Aspergillus, Mucormycosis, Cryptococcosis) | |
| Protozoan infections (Toxoplasmosis) | |
| Neuromuscular complications: | |
| Neuropathy | |
| Myopathy | |
| Neuromuscular junction disorders | |
| Seizures: | |
| Immunosuppressant toxicity | |
| Metabolic changes | |
| Infections | |
| Stroke | |
| Tumors | |
| Vascular neurologic complications: | |
| Posterior reversible encephalopathy syndrome (PRES) | |
| Ischemic stroke | |
| Intracerebral hemorrhage | |
| Reversible cerebral vasoconstriction syndrome | |
| Psychiatric and behavioral disorders: | |
| Depression | |
| Anxiety | |
| Bipolar disorders | |
| Psychosis | |
| Delirium | |
| Substance abuse | |
| Central nervous system post-transplant lymphoproliferative disorders (PTLD): | |
| Neurological complications of immunosuppressive agents: | |
| Other neurological manifestations: | |
| Altered consciousness and encephalopathy | |
| Central pontine myelinolysis | |
| Graft-versus-host disease | |
| Myelopathies | |
| Movement disorders | |
| Headache | |
| Visual and auditory disturbances | |
______
______
Infections and solid organ transplant rejection: a cause-and-effect relationship?
Although evidence is far from being conclusive, several studies have suggested that infections could trigger rejection in different transplant settings. There is evidence linking cytomegalovirus (CMV), adenovirus, enterovirus, parvovirus, and herpes simplex virus infections to the vasculopathy leading to cardiac allograft rejection; the association between CMV and chronic kidney, lung, and liver graft rejection; and the association of human herpesvirus 6 reactivation with CMV-related disease in kidney and liver transplant recipients. On the other hand, there are numerous antiviral prophylactic or pre-emptive treatments in use to control CMV infection, but they do not limit immune reactions leading to graft rejection or lower the risk of developing post-transplantation atherosclerosis in allograft recipients.
______
______
Organ trade, market and laws:
_
Can I sell an Organ?
More than 105,000 people in the U.S. are on a waiting list for a donated organ, but there are only about 15,000 donors each year. Thus, the high demand for organs creates an opportunity for those willing to sell a spare kidney, the lobe of a lung, or even the organs of the deceased. However, it is strictly illegal to sell an organ, in accordance with laws of most nations.
_
Illegal organ trade:
In the developing world, some people sell their organs illegally (on the black market), an underground practice that began in small quantities as early as the mid-1980s, as first reported on “60 Minutes” at that time. Then in following years, major newspapers in the U.S., and medical trade journal articles, began reporting an increased incidence of the practice. The incidence because so widespread and notorious, as often reported in “Nephrology News & Issues,” that federal legislation in the U.S. to ban the sale of organs and tissues, was proposed by Senator Al Gore, which became federal law in 1984, which was named the “National Organ and Transplant Act.” The federal legislation in the U.S. remains in effect to this day.
_
Transplant tourism:
According to WHO, “transplant tourism” refers to patients travelling across the borders to be transplanted elsewhere. People tend to travel for transplantation, either because it is not available in their home country, such as Tajikistan and Azerbaijan, or if the facilities are adequate in their home land, there are not enough organs available. Transplant tourism takes place in two different situations: 1) in very well developed countries with long waiting list, and 2) in underdeveloped countries with no prohibitory regulations for buying and selling the kidney, so people make money by selling their organs. According to Shimazono, transplant tourism refers to “overseas transplantation in which a patient obtains an organ through the organ trade or other means as organ trade may take other forms as well.” For example, Shimazono reported that live donors have been brought from the Republic of Moldova to the USA or from Nepal to India. In other cases, both recipients and donors from different countries move to a third country that contravenes the regulatory framework of their countries of origin.
_
Such potential human donors who are often living in India and Asia, routinely live in what is considered to be grave or extreme poverty and who are therefore exploited by profit-motivated salespersons who may take advantage of the donor’s desperate need to survive or pay for such basics as food, medical care and housing. The people who travel to make use of these kidneys are often known as “transplant tourists.” This practice is opposed by a variety of human rights groups, including Organs Watch, a group established by medical anthropologists, which was instrumental in exposing illegal international organ selling rings. These patients may have increased complications owing to poor infection control and lower medical and surgical standards. One surgeon has said that organ trade could be legalized in the UK to prevent such tourism, but this is not seen by the National Kidney Research Fund as the answer to a deficit in donors. In the illegal black market, the donors may not receive sufficient after-operation care, the price of a kidney may be above $160,000, middlemen take most of the money, the operation is more dangerous to both the donor and receiver, and the buyer often is infected with hepatitis or HIV. In legal markets of Iran, the price of a kidney is reported to be $2,000 to $4,000.
_
An article by Gary Becker and Julio Elias on “Introducing Incentives in the Market for Live and Cadaveric Organ Donations” said that a free market could help solve the problem of a scarcity in organ transplants. Their economic modelling was able to estimate the price tag for human kidneys ($15,000) and human livers ($32,000). Two books, Kidney for Sale By Owner by Mark Cherry (Georgetown University Press, 2005); and Stakes and Kidneys: Why markets in human body parts are morally imperative by James Stacey Taylor: (Ashgate Press, 2005); advocate using markets to increase the supply of organs available for transplantation. In a 2004 journal article Economist Alex Tabarrok argues that allowing organ sales, and elimination of organ donor lists will increase supply, lower costs and diminish social anxiety towards organ markets. Jason Brennan and Peter Jaworski of the CATO Institute have also argued that any moral objections to a market for organs aren’t inherent in the market, but rather, the activity itself. Now monetary compensation for organ donors is being legalized in Australia and Singapore. Kidney disease organizations in both countries have expressed their support.
_
China carrying out over 60,000 illegal organ transplants annually, a 2016 report finds:
The Chinese government continues to illegally harvest organs from millions of its innocent prisoners despite saying it had ended the practice two years ago, a decade-long study has alleged. Experts estimate between 60,000 and 100,000 organs are transplanted annually, and the majority of the hearts, livers and other organs are obtained by executing prisoners of conscience. In all, approximately 1.5 million transplants have taken place at 712 liver and kidney transplant centres across China since 2000, with over 300,000 of those taking place at unregulated centres. The report also found many surgeons had simply “lost count” of the quantity of transplants they had been asked to perform on a daily basis, with some having undertaken as many as six liver removals in one day.
_____
Organ Markets:
Two basic strategies have been proposed to provide incentives for people to sell their organs upon their death. One strategy is simply to permit organ sales by changing the National Organ Transplant Act (NOTA), the federal U.S. law that bans them. Then, individuals would be free to broker contracts with persons interested in selling at prices mutually agreed upon by both parties. Markets already exist on the internet between potential live sellers and people in need of organs, but these transactions are illegal. The other strategy is a regulated market in which the government would act as the purchaser of organs—setting a fixed price and enforcing conditions of sale. Both proposals have drawn heated ethical criticism.
_
One criticism is that only the poor and desperate will want to sell their body parts. If you need money, you might sell your kidney to try and feed your family or to pay back a debt. This may be a “rational” decision, but that does not make it a matter of free choice. Watching your child go hungry when you have no job and a wealthy person waves a wad of bills in your face is not exactly a scenario that inspires confidence in the fairness of a ‘free’ market for body parts. Talk of individual rights and autonomy is hollow if those with no options must “choose” to sell their organs to purchase life’s necessities. This scenario has manifested in Iran, where the sale of organs is legal. In that country there is virtually no waiting list, yet it appears some individuals compete to sell their organs at low prices to feed their families. Coercion is rampant, including instances in which the organ “buyer” lowers the offer at the last minute, and the “seller” must choose between accepting the new terms and the ability to provide for their family a little longer. Choice requires information, options, and some degree of freedom, as well as the ability to reason.
_
It is hard to imagine many people in wealthy countries eager to sell their organs upon their death. In fact, even if compensation is relatively high, few will agree to sell. That has been the experience with markets in human eggs for research purposes and with paid surrogacy in the U.S.—prices have escalated, but there are still relatively few sellers. Some maintain that selling organs, even in a tightly regulated market, violates the ethics of medicine. The doctor harms the patient for no end other than a sale to another party. The core ethical norm of the medical profession is the principle, “Do no harm.” The only way that removing an organ from someone seems morally defensible is if the donor chooses to undergo the harm of surgery solely to help another, and if there is sufficient medical benefit to the recipient. The creation of a market puts medicine in the position of removing body parts from people solely to abet their interest in securing compensation. A market in human organs has a model in the existing market for human eggs for assisted reproduction and research purposes, but that practice is highly controversial. Is this a role that the health professions can ethically countenance? In a market—even a regulated one—doctors and nurses still would be using their skills to help people harm themselves solely for money. The resulting distrust and loss of professional standards may be too high a price to pay to gamble on the hope that a market may secure more organs for those in need.
_____
The kidney trade in India:
Organ transplantation in India has received prominent coverage in the media, one major reason being the notorious kidney trade in the 1980s. Foreign patients flocked to India for transplants from paid “donors”. These transplants were often performed clandestinely in small hospitals in substandard conditions, but some large private institutions tacitly participated in this activity. The results of these transplants were also poor. While the media reported on these scandals, medical bodies, including medical councils and other regulatory bodies, largely remained silent. This was not surprising considering that self-regulation of medical practice in India has historically been very weak. Also, the kidney trade earned huge monetary benefits for the rapidly expanding private sector. A significant section of the medical fraternity, including nephrologists and kidney transplant surgeons, was complicit in the kidney trade. Attempts were made to offer an ideological rationale for this activity, seeking to justify paid-for donations as consistent with a libertarian and free market philosophy. Using the same logic, there were calls for a “regulated” market. It was, however, obvious on the ground level that the donors in this market had often been coerced and even been duped by middlemen of any monetary rewards. Also, follow-up studies of unrelated donors showed that their quality of life was poor. Countries like Iran have experimented with a state-sponsored regulated model and claimed some success.
_
The Transplantation of Human Organs Act India:
Partly as a response to the kidney scams, the Central government in 1991 constituted a committee to prepare a report which could form a basis for all-India legislation governing organ transplantation. Although the main terms of reference of the committee were concerned with “brain death”, it also recommended that trading in human organs be made a punishable offense. In 1994, the government of India promulgated the Transplantation of Human Organs Act (THOA). The Transplantation of Human Organs Rules followed in 1995. Subsequently the Rules alone were amended in 2008. Later, THOA itself was amended in 2011.The Rules for the amended Act have just been notified, in 2014. THOA of 1994 banned any form of “commercial trading” in organs. Unrelated donation was permitted on grounds of altruism but only with the sanction of an authorisation committee. The committee took a decision on the basis of documentation and interviews of both prospective donor and recipient. Even after the promulgation of THOA, scandals involving unrelated donors continued to break out in the media. In the last few years there seems to have been a decrease in media exposes. This may reflect an overall reduction in what was once a thriving industry, but it is also believed that some of the activity has moved underground, and some has moved out of the country where the wealthy and influential have taken advantage of the apparently liberal laws in countries like Singapore and undergone live unrelated transplantation there. Simultaneously, THOA also legalised brain death in India, paving the way for performing deceased donation by procuring organs from brain stem dead donors. The Act also laid down criteria for determining brain death. Safeguards against misuse were built into the rules. The tests for brain death had to be performed together by four individuals, none of whom had anything to do with the transplant. The tests were to be done twice, with a minimum gap of six hours. As per the law, brain death could be declared only in institutions recognised by the state appropriate authority. Written consent for donation of organs from the deceased person had to be obtained only from a close relative. The law and most of the scientific criteria and the methodology of diagnosing brain death were essentially derived from the British law. THOA laid down elaborate criteria on who can donate organs, but did not elaborate on how the donated organs would be distributed. Conceptually, donated organs do not belong to the hospital or the city where the donor’s death took place; all altruistic donations belong to society as a whole. Thus the state has a responsibility to ensure that such organs are distributed in a transparent and equitable manner to those who need them, and not to those who can afford them. If they leave the decision to market forces, the state and the transplant community are breaching the trust placed in them by donor families.
_____
Transplant laws:
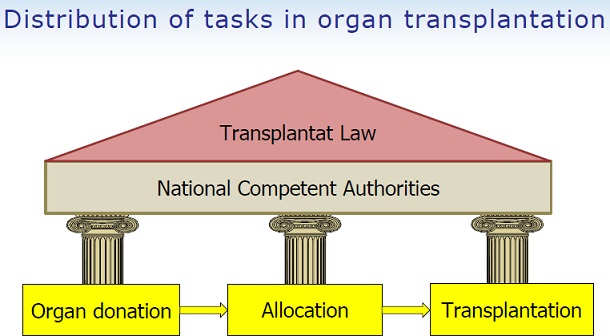
Both developing and developed countries have forged various policies to try to increase the safety and availability of organ transplants to their citizens. Austria, Brazil, France, Italy, Poland and Spain have ruled all adults potential donors with the “opting out” policy, unless they attain cards specifying not to be. However, whilst potential recipients in developing countries may mirror their more developed counterparts in desperation, potential donors in developing countries do not. The Indian government has had difficulty tracking the flourishing organ black market in their country, but in recent times it has amended its organ transplant law to make punishment more stringent for commercial dealings in organs. It has also included new clauses in the law to support deceased organ donation, such as making it mandatory to request for organ donation in case of brain death. Other countries victimized by illegal organ trade have also implemented legislative reactions. Moldova has made international adoption illegal in fear of organ traffickers. China has made selling of organs illegal as of July 2006 and claims that all prisoner organ donors have filed consent. However, doctors in other countries, such as the United Kingdom, have accused China of abusing its high capital punishment rate. Despite these efforts, illegal organ trafficking continues to thrive and can be attributed to corruption in healthcare systems, which has been traced as high up as the doctors themselves in China and Ukraine, and the blind eye economically strained governments and health care programs must sometimes turn to organ trafficking. Some organs are also shipped to Uganda and the Netherlands. In an article appearing in the April 2004 issue of Econ Journal Watch, economist Alex Tabarrok examined the impact of direct consent laws on transplant organ availability. Tabarrok found that social pressures resisting the use of transplant organs decreased over time as the opportunity of individual decisions increased. Tabarrok concluded his study suggesting that gradual elimination of organ donation restrictions and move to a free market in organ sales will increase supply of organs and encourage broader social acceptance of organ donation as a practice.
_
The German Transplant Act (TPG):
In Germany, transplantation of human organs is governed by the Act on “organ and tissue donation, removal and transplantation” (Gesetz über die “Spende, Entnahme und Übertragung von Organen und Gewebe” or: Transplant Act – TPG). The Act was passed by the German Bundestag on 5 November 1997 and came into force on 1 December 1997; an amended version was published on 4 September 2007 and on 1 August 2012. Depending on whether the organs were donated after the death of the donor or taken from a living one, the act prescribes different regulations.
_
The National Organ Transplant Act in the U.S.:
Under the National Organ Transplant Act of 1984 (NOTA), any individual convicted of buying or selling human organs faces a five-year prison sentence and/or a hefty fine. Since the language of the law explicitly states that it is a crime for an individual to “knowingly acquire, receive, or otherwise transfer” a human organ, it allows safe harbor for those who unknowingly receive an illegally procured organ. But, while you may not profit from donating an organ, you may have some of your expenses related to the donation procedure reimbursed. For example, you may claim medical costs and missed pay following the donation of an organ. Different states calculate such payments differently, but anything considered to be unreasonable will not be reimbursed. Specifically, the law states, payment of “expenses of travel, housing, and lost wages incurred by the donor of a human organ in connection with the donation of the organ” is permitted. However, living donors (those donating a single kidney or a portion of an organ) may not be reimbursed for some of the associated post-operative costs. Also, living donors may experience difficulty maintaining affordable health insurance coverage after such a procedure. Most transplant centers offer the assistance of financial coordinators to help with insurance and related issues. Some states offer additional reimbursement to the families of deceased organ donors. In sum, while you cannot sell an organ, you may be fairly compensated for some costs related to your donation
____
There are other areas of inquiry:
(1) Legal regulation of transplanting suboptimal organs:
A shortage of suitable organs and the growing number of patients dying on transplant waiting lists have necessitated increasing use of less-than-ideal organs from deceased donors. This includes organs from older donors or those with co-morbidities, infections, current or previous cancers or history of high risk behaviour such as smoking, excessive alcohol and illicit drug use. The outcomes from transplantation of such ‘suboptimal’ organs are generally acceptable for the patient population compared to the even greater risk of death while waiting for an organ. However, compared to optimal organs, transplantation of sup-optimal organs exposes individual patients to greater risk of transmission of disease and major morbidity, graft loss or death. This necessitates the development of effective approaches that address not only the medical issues, but also the fundamental legal and ethical issues in the use of suboptimal organs.
(2) Legal considerations on pre-mortem interventions in donation after circulatory death:
The proportion of organs transplanted following donation after circulatory death (DCD) has steadily increased in the UK and is approaching that from donation after brain death (DBD). Because death must be declared after cessation of circulation following withdrawal of life-supporting treatment, DCD organs are necessarily exposed to a period of warm ischaemia before they can be perfused with cold preservation solution. This has significant deleterious effects on graft and patient outcomes after transplantation. The detrimental impact of warm ischaemia in DCD donors can potentially be ameliorated by pre-mortem treatments of the donor, such as systemic anticoagulation. However, such interventions are currently prohibited by UK law whereas they are permissible in the US. UK regulations stem from the legal definition of death and prohibition of interventions that are not directly intended to benefit the donor before declaration of death.
____
____
Ethics in organ donation and transplantation:
Nearly all scholars and societies around the world agree that voluntarily donating organs to sick people is ethically permissible. Although nearly all scholars encourage organ donation, fewer scholars believe that all people are ethically required to donate their organs after death. Similarly, nearly all religions support voluntary organ donation as a charitable act of great benefit to the community, although a few small groups, like the Roma (gypsies), oppose organ donation on religious grounds. Issues surrounding patient autonomy, living wills, and guardianship make it nearly impossible for involuntary organ donation to occur. The primary issues surrounding the morality of organ donation are semantic in nature. The debate over the definitions of life, death, human, and body is ongoing. For example, whether or not a brain-dead patient ought to be kept artificially animate in order to preserve organs for donation is an ongoing problem in clinical bioethics. In addition, some have argued that organ donation constitutes an act of self-harm, even when an organ is donated willingly. Further, the use of cloning to produce organs with a genotype identical to the recipient is a controversial topic, especially considering the possibility for an entire person to be brought into being for the express purpose of being destroyed for organ procurement. While the benefit of such a cloned organ would be a zero-percent chance of transplant rejection, the ethical issues involved with creating and killing a clone may outweigh these benefits. However, it may be possible in the future to use cloned stem-cells to grow a new organ without creating a new human being.
_
The existence and distribution of organ transplantation procedures in developing countries, while almost always beneficial to those receiving them, raise many ethical concerns. Both the source and method of obtaining the organ to transplant are major ethical issues to consider, as well as the notion of distributive justice. The World Health Organization argues that transplantations promote health, but the notion of “transplantation tourism” has the potential to violate human rights or exploit the poor, to have unintended health consequences, and to provide unequal access to services, all of which ultimately may cause harm. Regardless of the “gift of life”, in the context of developing countries, this might be coercive. The practice of coercion could be considered exploitative of the poor population, violating basic human rights according to Articles 3 and 4 of the Universal Declaration of Human Rights. There is also a powerful opposing view, that trade in organs, if properly and effectively regulated to ensure that the seller is fully informed of all the consequences of donation, is a mutually beneficial transaction between two consenting adults, and that prohibiting it would itself be a violation of Articles 3 and 29 of the Universal Declaration of Human Rights. Even within developed countries there is concern that enthusiasm for increasing the supply of organs may trample on respect for the right to life. The question is made even more complicated by the fact that the “irreversibility” criterion for legal death cannot be adequately defined and can easily change with changing technology.
_
Transplantation represents one of the best examples of the scientific achievements of medical science. However, its success has also led to some of the fiercest ethical challenges in modern medicine. The number of patients desperately needing a transplant far outnumbers the available organs, leading to a competition for organs which severely tests the principles of transparency and distributive justice. Transplantation is also unique in that it needs public sanction without which it will collapse. Although living donation is an option for some organs, the main source of organs is deceased donation which hinges on consent from family members. This consent is shaped not only by the perceived credibility of the process but also by other cultural, religious and political factors. On the recipient side, the ethical challenge is how to ensure justice in allocating the few available organs to someone from amongst a large pool of patients on a waiting list. The discourse surrounding organ transplantation covers a wide sweep of disciplines like sociology, anthropology, culture studies, public health, economics and politics. Central to the discussion, however, is ethics. Over the years this discipline has engaged with these debates in an intense and rigorous manner.
_
The ethical questions raised by organ transplantation are multiple and complex. Three main issues related to organ transplantation include the fundamental morality of transplanting body parts, the ethics of organ procurement, and the ethics of allocation. Does organ transplantation involve too much control of nature, and lead to scenarios of “playing God”? The technological and medical advancements associated with organ transplantation have saved the lives of many, but scarce organ resources have contributed to many social issues regarding allocation. There are over 100,000 candidates on the waiting list in the United States, and the organ supply is scarce. Who should get the available organs, and by what criteria should this decision be made?
_
The shortage of organs available for transplant gives rise to moral and ethical issues surrounding the procurement and distribution organs:
- Should those who have a better chance for survival be given priority over other patients needing organ transplants?
- Should parents of young children be given priority?
- Should those whose lifestyle choices (smoking, drinking, drug use, obesity, etc.) damaged their organ(s) be given the opportunity of an organ transplant?
- Should incentives, either monetary or non-monetary, be offered in order to encourage organ donation? Should those who made the decision to donate organs of a loved one who has been declared dead receive any kind of financial compensation?
- Does “transplant tourism” – the concept of traveling to developing countries to obtain organs exploit the poor and what does this mean for distributive justice?
- Should prisoners on death row be given the option of donating organs upon their death, or even be offered the option of trading a kidney or bone marrow in exchange for a life sentence in prison without parole?
- Should everyone be required to indicate their wishes regarding organ transplantation on either their income tax forms or driver’s license?
- Should consent to donate organs be presumed, so that organs are donated unless a person, while still living, specifically requests not to donate upon death?
- Should organs be created through the use of stem cells?
- Should hospital policies permit organs to be taken from non- heart-beating donors (NHBD) to increase the number of organs available?
_
Why should donors and donor receiver’s be anonymous?
The reason why anonymity is practiced is that the relationship between donor and receiver can be a difficult one especially for the families concerned. We have seen unfortunate examples of difficulties experienced in various countries. Both parties may have different motivations: receivers often have a desire to express gratitude and continue to live their lives, while the donor’s next-of-kin may build a lifelong relationship with the receiver of the donor as a consolation of their loss. This can be a psychological burden for both parties. For this reasons it is recommended that those receiving a transplant or the relatives of the organ donor(s) do not release the exact time of transplantation. The season and time of year is ok.
_
Should the Definition of Death be changed?
Most donated organs now come from people declared dead on the basis of neurological criteria—the absence of brain activity. Brain death typically occurs before cardiopulmonary death, the cessation of a heartbeat and breathing. One way to expand the pool of deceased donors is to include those declared dead by cardiopulmonary criteria. This recommendation was made in 2006 by a panel of the Institute of Medicine chaired by Hastings Center fellow James F. Childress and including Hastings fellow Mary Ann Baily.
_
Donation after circulatory death (DCD) has become more common around the world, but the practice is controversial. For one thing, it is medically more complex than donation after brain death because of the risk of organs being harmed by oxygen deprivation. In addition, there is ethical concern that DCD will lead to substandard health care at the end of life—for example, inadequate morphine in the effort to avoid harming the organs. The Institute of Medicine report recommends ethical guidelines already used in Europe, such as preventing the organ recovery team from being the ones to decide when to discontinue cardiopulmonary resuscitation.
_
An extension of DCD is the procurement of organs from people who die unexpectedly, often not in a hospital, which is called “uncontrolled donation after circulatory death” (uDCD). Teams in Spain and France have shown that uDCD can contribute to improved transplantation rates with good outcomes. Progress in organ containment and transportation methods help protect against lengthy time without oxygen, a risk in uncontrolled settings, such as the scene of a motor vehicle accident. Some fear that uDCD would lead to reduced efforts to save lives in favor of procuring organs, or that death would not be accurately confirmed prior to procurement. These concerns might be assuaged by policies such as one proposed in New York City that would require 30 minutes of vigorous resuscitation effort by trained EMTs, which would terminate only after futility standards have been met (including impossibility of restarting cardiac and respiratory function, and spontaneous circulation). After termination, the patient would be declared dead and then permission would be sought to transfer the body to a hospital so that organ donation could be considered. Under such a two-step protocol, those responsible for determining death would be completely separate from those assessing feasibility of donation, and there would be time for the deceased’s prior consent to donate to be verified.
_
The controversy surrounding Organ Donation:
What makes organ donation a controversy? This can be due to several factors impacting organ donations such as the culture, the public opinion on organ donation, religious reasons, and fear and misconceptions concerning the process. The surgeons performing organ harvests are completely different from the physicians treating you, and also, there is no shortage of people dying and hence no reason to not give you the treatments you need, assuming you are a full code. Another question people ask, how do the doctors know the patient is truly dead? There are two main reasons. First, organ donors are given additional tests to ensure that the donor truly is dead. Second, the clinical definition of death is either brain death (the complete and irreversible loss of all brain function) or circulatory death (the irreversible loss of function of the heart and lungs). Timing is a vital aspect to ensure that the tissues can be considered viable for transplants, and the physicians do not withdraw care on their own to meet those criteria. There would be a discussion with the family to talk about the situation and choices that have to be made. Then it would proceed from there. For each patient, the care and respect for the end of life process is highly regarded and will always be held to a high standard, whether or not they are organ donor.
______
______
Religious viewpoints:
All major religions accept organ donation in at least some form on either utilitarian grounds (i.e., because of its life-saving capabilities) or deontological grounds (e.g., the right of an individual believer to make his or her own decision). Most religions, among them the Roman Catholic Church, support organ donation on the grounds that it constitutes an act of charity and provides a means of saving a life, consequently Pope Francis is an organ donor. One religious group, The Jesus Christians, became known as “The Kidney Cult” because more than half its members had donated their kidneys altruistically. Jesus Christians claim altruistic kidney donation is a great way to “Do unto others what they would want you to do unto them.” Some religions impose certain restrictions on the types of organs that may be donated and/or on the means by which organs may be harvested and/or transplanted. For example, Jehovah’s Witnesses require that organs be drained of any blood due to their interpretation of the Hebrew Bible/Christian Old Testament as prohibiting blood transfusion, and Muslims require that the donor have provided written consent in advance. A few groups disfavor organ transplantation or donation; notably, these include Shinto and those who follow the customs of the Gypsies. Orthodox Judaism considers organ donation obligatory if it will save a life, as long as the donor is considered dead as defined by Jewish law. In both Orthodox Judaism and non-Orthodox Judaism, the majority view holds that organ donation is permitted in the case of irreversible cardiac rhythm cessation. In some cases, rabbinic authorities believe that organ donation may be mandatory, whereas a minority opinion considers any donation of a live organ as forbidden.
_____
_____
Challenges to ODT:
Over the course of the last century, organ transplantation has overcome major technical limitations to become the success it is today. The breakthroughs include developing techniques for vascular anastomoses, managing the immune response (initially by avoiding it with the use of identical twins and subsequently controlling it with chemical immunosuppressants), and devising preservation solutions that enable prolonged periods of ex vivo storage while preserving function. One challenge that has remained from the outset is to overcome the shortage of suitable donor organs. The results of organ transplantation continue to improve, both as a consequence of the above innovations and the improvements in peri- and postoperative management.
_
The major challenges in the field of solid organ transplantation are the organ shortage and achieving tolerance. Dr. Flavio Vincenti, Professor, Division of Nephrology, University of California, San Francisco, does not foresee any near-term resolution to the organ shortage but believes the field is making gains in achieving operational rather than immunologic tolerance. Other unmet needs facing the transplant community include treatment of antibody mediated rejection, ischemia-reperfusion injury and immune monitoring. He reviews the most significant challenges facing the transplant field and discusses developments underway to improve patient monitoring and therapy. Important challenge in improving outcomes is to prevent and minimize ischemia reperfusion because an increasing proportion of kidneys are obtained from Expanded Criteria Donors (ECD) and donors after cardiac death (DCD). These kidneys have a higher risk of graft loss when compared to kidneys transplanted from standard criteria donors. We want to minimize the higher rate of delayed graft function in these kidneys and reduce morbidity which may occur during the period of delayed graft function.
_
Organ transplantation is a unique form of therapy for organ failure. The results are overall extremely good, saving the lives of a large cohort of patients that would otherwise die or be left with reduced life expectancy and a poor quality of life. Yet, the success of transplantation creates a problem that is increasingly difficult to manage, – the shortage of organ grafts available for transplantation. Simultaneously, the average age of deceased donors increases in most western countries, and a high prevalence of life-style associated diseases like obesity, diabetes and hypertension impacts organ quality. Various strategies have been applied to cope with the ever-increasing demand for organs. Extended criteria grafts can in many instances be used successfully if transplanted to properly selected recipients, but are associated with an increased risk of short and long-term graft loss due to poor function. Donation after circulatory death as an adjunct to donation after brain death have been successfully introduced in many countries and currently contributes to a significant part of all organs transplanted in Europe and the US. Both strategies have raised the need for close monitoring of organ function and therapeutic measures to improve organ quality. Machine perfusion of organs could be a way to both reduce the negative impact of ischemia but moreover as an innovative strategy for reducing the ischemia-reperfusion injury at revascularization. Ultimately the concept of using ex-vivo perfusion as a way to achieve reconditioning of organs in order to convert “non-transplantable organs” into acceptable grafts has emerged. The approached was pioneered in Lungs by Steen and coworkers in Sweden in 2007. Recently, a similar approach has been reported in liver transplantation. The significant progress seen in organ preservation and possible reconditioning over the recent years has even made heart transplantation after circulatory death possible. The concerted efforts of the transplant community to find new innovative strategies to alleviate organ shortage is a result of continuous and systematic work, and clearly demonstrates the importance of scientific medicine in improving the treatment and care for our patients. The emergence of paired donor exchange networks as very important, since they allow transplantation in individuals who would otherwise have difficulty finding suitable matches long-term. Finally there is promising field of regenerative medicine. The use of decellularized xenografts, that are re-populated with the recipient induced pluripotent stem cells, offers the hope that we can both address the organ shortage and that we can do so with organs that are fully tolerated by the recipient, because we’re using their own cells.
_____
_____
Consent for organ donation:
Organ transplants generate increasingly vexing legal and ethical questions as medical technology becomes more complex. Three controversial issues surrounding the subject are conception for organ donation, donor consent, and transplants from terminally disabled infants.
_
Methods of obtaining consent for organ donation after death:
There are two main methods for determining voluntary consent for organ donation after death. One of them is the “opt in” method by which only those who have given explicit consent are donors. The second method is the “opt out” or “by default”, which assumes that anyone who has not refused is a potential donor. It has been established that opt-out legislative systems dramatically increase effective rates of consent for donation. Germany, the UK and the US have adopted an opt-in system. Germany, for example, has an organ donation consent rate of 12% among its population. By contrast, Austria, its neighboring a country with a very similar culture and economic development, has a consent rate of 99.98%. Austria, as well as Spain – world leader in organ donations and transplants- and Belgium, have adopted an opt-out system which entails “presumed consent” from the deceased donor. In the opt-out system, it is the deceased next of kin who ultimately make the decision on organ donation. Many claim however that, the opt-out or by default method does not solve the problem. Instead to really improve the current rates of organ donation after death, it should be made compulsory regardless of the deceased or the family consent and even if this goes against the person’s religious beliefs. Supporters of compulsory donation claim that a person’s right to live through organ transplantation is more important than the right of deciding what to do with the organs of a dead person.
_
Presumed Consent (opt-out system):
This is another option for increasing the organ supply that has not been tried in the U.S. but is practiced abroad. Spain, Italy, Austria, Belgium, Hungary, Croatia, and many other European countries have enacted laws that create presumed consent, or what we prefer to call “default to donation.” In such a system, the presumption is that you want to be an organ donor upon your death—the default to donation. People who don’t want to be organ donors have to say so by registering this wish on a computer, carrying a card, or telling their loved ones. With default to donation, no one’s rights are taken away—voluntary altruism remains the moral foundation for making organs available, and, therefore, procuring organs is consistent with medical ethics. Based on the European experience, there is a good chance many regions in America could get a significant jump in the supply of organs by shifting to a default-to-donation policy. Donation rates in some European countries with presumed consent are about 25% higher than in other European nations.
_
Default to donation proposals have been submitted in several states over recent decades, but they have yet to be adopted anywhere in the U.S. As of 2015, Wales became the first nation in the U.K. to adopt presumed consent, with about 86,000 people (3% of the population) opting out shortly after implementation of the law. If Welsh families know that the deceased did not want to donate, despite lack of documentation, their expression to this effect will prevent procurement. Scotland and Iceland are instituting presumed consent as well. If these policies are successful, they may provide momentum for trying default to donation elsewhere in the U.K. and in the U.S.
_
There are important issues to consider before moving to default to donation. For millions of people who are used to actively deciding for or against donation when registering at the DMV or online, a shift to presumed consent could be unsettling. To preserve fairness and trust, an education campaign designed to reach everyone affected must accompany the legislation. The role of the family would also need to be clear: Should families have no say, or should they be able to veto default to donation of a deceased relative based on knowing the person’s unwritten wishes? Or, since the family has to keep living knowing a loved one’s organs are in a new person—and might find that knowledge distressing–should they have unqualified veto power? These questions also bring to bear the fact that in nearly all countries with presumed consent laws, donation professionals almost always still seek family consent as if they were in an opt in system.
_
The main ethical objection to presumed consent is the perceived loss of patient autonomy–that it is wrong to take someone’s organs without that person’s explicit consent. In addition, some people believe that presumed consent violates the 5th Amendment prohibition against taking private property without due process and compensation. Critics are also concerned about mistakes in which there is the presumption that someone consented when, in fact, either the individual meant to indicate opposition but had failed to do so or the record of that opposition was lost. Critics also claim that a presumed consent system is expensive to create and maintain. It requires the creation of large, centralized registries listing individuals’ decisions regarding their own body, and these must be updated continuously. Mistakes inevitably occur, causing unwanted organ removal and expensive lawsuits. Those who find fault with the ethical premise of presumed consent argue that it removes the moral dignity surrounding donation by making it mandatory. It also detracts from the goal of free choice and autonomous behavior by precluding the individual from making no decision or from leaving the decision to others.
_
Do Defaults Save Lives? A 2003 study:
Since 1995, more than 45,000 people in the United States have died waiting for a suitable donor organ. Although an oft-cited poll showed that 85% of Americans approve of organ donation, less than half had made a decision about donating, and fewer still (28%) had granted permission by signing a donor card. The data from this study and those of Gimbel et al. suggest changes in defaults could increase donations in the United States of additional thousands of donors a year. Because each donor can be used for about three transplants, the consequences are substantial in lives saved. These results stand in contrast with the suggestion that defaults do not matter. Policy-makers performing analysis in this and other domains should consider that defaults make a difference.
_
An international comparison of deceased and living organ donation/transplant rates in opt-in and opt-out systems: a panel study: 2014
While the number of deceased donors is higher than the number of living donors, opt-out consent leads to a relative increase in the total number of livers and kidneys transplanted. The results show that opt-out consent may lead to an increase in deceased donation but a reduction in living donation rates. Opt-out consent is also associated with an increase in the total number of livers and kidneys transplanted.
______
Required Request Program:
A required request program is a more moderate approach to the problem of organ donation. It seeks to reform the existing system of encouraged voluntarism by requiring that family members or guardians be given the opportunity to make an organ donation when a death has occurred. Such a program would require hospitals to have a specially trained person to approach families and inquire about organ donation at the time death is pronounced. The request would be noted in writing on the death certificate to ensure that medical providers comply with the policy. The required request system would allow for exceptions in cases where a request would not be in the best interests of family members or guardians, with such exceptions also duly noted on the death certificate. Such a system, its advocates claim, would increase freedom of choice by informing individuals of their options. Proponents of this system point to statistics that indicate that in the U.S. public, the level of altruism regarding organ donation is quite high. In some hospitals, for example, over 60 percent of the families who were asked to donate the organs of loved ones agreed to do so. The problem with the current system, they maintain, is that donor cards (opt-in system) do not adequately tap this altruistic sentiment. They also note that a required request system would ensure that donor cards or written directives are honored. With time, such requests would become a routine part of the death process in medical facilities, making them less surprising and less intrusive to family privacy at the time of death. Critics of the required request system say that it would not do enough to change an already flawed organ procurement system. Moreover, they argue that approaching families in the hours following the death of a loved one imposes too much psychological distress.
_____
Why do families refuse to give consent for donation?
Understanding this complex question is a key issue if low consent rates are to be increased. Some work has attempted to address this as a primary research goal. By their nature, most studies are observational and qualitative in design. Although grounds for refusal may have a basis in strong local cultural and religious beliefs in certain countries, there are many common themes to be found worldwide. The most frequent reasons that emerge, but by no means an exhaustive list, are shown in Table below.
_
Common reasons for family refusal to consent for organ donation:
| Reason |
| Relatives not wishing surgery to the body/concerns regarding disfigurement |
| Feelings that the patient had suffered enough |
| Uncertainty regarding the patient’s wishes |
| Disagreements among the family group |
| Religious/cultural reasons |
| Dissatisfaction with healthcare staff and process |
| Concerns over delay to funeral/burial process |
| Unable to accept death, lack of understanding of brain death |
| Concerns regarding integrity of process, e.g. unfair organ allocation, organ selling |
| Relatives had decided on their own that organs would not be suitable |
| Longstanding negative views on organ donation |
| Relatives were emotionally exhausted |
_
Other groups have attempted to describe the complex and conflicting emotional responses to death and requests for organ donation in a different way, concentrating on innate psychological responses and the modelling thereof. Sque and colleagues performed a fascinating interview study of the family members of 23 potential organ donors who had all declined consent. They identified an essential conflict between the ‘gift of life’ (the prevailing view of healthcare professionals and perhaps society) and the ‘sacrifice’ required at both a personal emotional (relief of ‘guardianship’ and ‘protection of the body’) and physical (perceived mutilation to an otherwise viable looking body) level. In the case of DBD, this group describes an emotional ‘dissonance’ set up by a failure to resolve a poor understanding of brain death and the proposed donation procedure. Other important innate responses include the perceived relation between ‘body’ and ‘self’ (strong belief in some that the physical body is inherently part of identity), and common ‘death anxiety defences’ including the ‘feeling of immortality’ reinforced by the appearance of a still warm well-perfused potential brain-dead donor. It is suggested that in some individuals, such responses overcome the more rational or altruistic motives necessary for consent.
_
Potential organ donor must convey his/her decision to donate organ after death to their families as almost 90% of families agree to organ donation if they know their relative’s decision but this falls to less than 50% if they haven’t had the conversation.
_______
_______
Organ shortage:
As organ transplants became increasingly successful, the most significant problem related to them was the shortage of available organs. A large gap separated the high demand for organs and their scarce supply. Experts estimated that by the late 1980s, three people were on transplant waiting lists for every available organ. Given the grossly inadequate supply of organs, many vexing ethical, legal, and political issues surrounded the question of what is the best way to harvest or procure organs. In the early days of organ transplant surgery, during the 1960s and 1970s, the practice was seen as experimental and risky. Patients’ bodies often rejected a transplant, and the survival rate in many cases was deemed too low to be acceptable. However, with the development of new surgical procedures and the wide use of new immunosuppressive drugs such as cyclosporine in the 1980s, organ transplantation became a common medical technique available to more and more people. In the 1980s, over 400,000 transplants were performed in the United States. The age range of heart transplant recipients has expanded from forty-five to over sixty at the upper limit, and to infancy at the lower limit. Results such as these have caused such a demand for organ transplants that there are far more potential organ recipients than available organs. Those who are deemed medically suitable to receive organs are put on long waiting lists, and it is often months or years before they get the organs they need; many others are deemed medically unsuitable and are not even put on waiting lists. Some have criticized the term medically unsuitable as an arbitrary and uncertain medical judgment used simply to prevent raising the hopes of those who are unlikely to get a timely transplant. What should be done about this dire shortage of organs available for transplantation? Three different organ procurement systems have been proposed as a means of alleviating the situation: an organ market, a presumed consent program, and a required request program. All three proposals have their advocates and detractors.
_
In the United States every ten minutes someone is added to the national organ transplant waiting list. While waiting for a transplant an average of 20 people die each day in the US, while 450 people die annually in the U.K. waiting for an organ donation. Some 4,000 people die annually across the European Union waiting for organ donation. And at the same time, these statistics do not tell the whole story of how many die from not receiving donor organs in these areas. Those specifics are even more sad. There are additional people who do not qualify for being put on those donor lists at all due to being bad candidates for transplants. There are others who would want to receive an organ but who do not qualify as being among those patients with the highest need. Yet other may not qualify as the most qualified recipient according to government regulations or trade organization regulations about who should get a transplant. There are additionally people who never make it onto the donor list because the odds of them getting a transplant quickly enough are too low. In some situations, this is a level of hopelessness that some doctors don’t consider to even be worth the paperwork required to place the patient on an organ donation list, and the doctor consequently shares that hopelessness with the patient through a few choice words of discouragement. It’s a far worse situation than the official numbers indicate, but the lack of much needed organs is a problem with a solution.
_
The shortage of organs is a major problem worldwide. There are many more patients awaiting transplantation than there are organ donors. The shortage of organ donors is multifactorial. In general, the number of potential donors that meet the criteria of a brain death diagnosis is far greater than the number of utilized donors where transplantation took place. The difference between these numbers is due to medical and logistic factors, the ability to determine brain death, and cultural and religious factors that affect the willingness of the population to donate organs. As a result of these factors, there is a large variability in organ donation rates among countries, and, therefore, the waiting time for transplantation is largely variable. Shortage of organs should be analyzed separately for living and deceased donors. For deceased donor programs the most important factor is the availability of a sound national or regional transplantation program that meets international standards. According to the World Health Organization (WHO) criteria, such a program should be present in each country, so that it becomes self-sufficient over time with respect to its population organ needs. An important factor is the cultural compliance and general consent of the society to organ donations. There are many and variable ethical and religious issues related to organ donation. While in all major religions organ donation is encouraged in order to save lives, there may be huge differences in the practical approaches to the donation process among different factions even within the same religion.
_
Currently, in the U.S., there is a growing disparity between the organ donor list and the organ transplant waiting list. The statistics are clear, 95% of U.S. adults support organ donation, but not nearly enough sign up to be donors. Additionally, even less are available as only about 0.3% of people die in a way to allow organ donation. In order to have your organs considered for transplants, the organs have to be maintained on artificial support systems, meaning that if an organ donor does not make it to a hospital before they die, they cannot become an organ donor. The system in the U.S. requires people to opt-in to become an organ donor, either online or when you are renewing your driver’s license at the DMV. Having an organ donor card isn’t necessarily enough as those may be misplaced or lost, and it is recommended to sign up for your state’s donor registry and tell family and friends so that they may let the medical professionals know your wishes. However, the waiting list is only getting bigger and bigger as seen in the figure below.
_
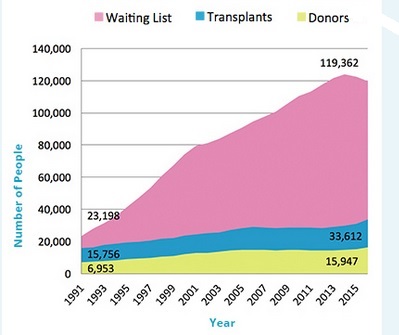
Graph above shows the difference between the number of people on organ transplant wait list, number of people getting transplants, and the number of organ donors in the United States.
___
Reasons for Organs Shortage:
The myriad reasons of shortage are administrative, legal, health system, and knowledge, attitude, and practice gap of stakeholders. Contrary to many studies, cultural, social, educational issues, language barrier, and religious concerns do not play a significant role in the decision for or against donation. Some of the specific reasons for organ shortage are:
- Fear of death and surgical mutilation
- Lack of awareness of brain death concept among medical professionals and public
- A misapprehension about brain death
- Fear to declare patient dead even before they are actually dead
- Religious fallacies
- Out-of-pocket expenses
- Lack of system regarding identification and maintenance of brain dead donors
- Socio-cultural beliefs including desire to be buried/burnt completely and re-birth without a missing organ
- Mental non-acceptance of idea living with another person’s organ say kidney
- Lack of government support
- Public and professionals attitude to brain death and Organ donation
- Lack of system transparency and perception of misuse of organs
- Dynamics of decision making for actual donation
- Poor funding and budget due to competing need/demand
- Inadequate health insurance
- Adverse media reporting and negative publicity
- Legal, administrative/bureaucratic, and equity issues
- Non-availability of trained transplant coordinators/counselors
- Hospital infrastructure, logistics, manpower, functional linkage, and support system
_
Factors contributing to organ shortage, a study:
Ironically, the single largest factor in today’s donor organ shortfall is that solid organ transplants have become so successful. Improved survival rates and the expectation that organ replacement will enhance quality of life have encouraged more doctors and their patients with organ failure to opt for transplantation.
The study also identified a number of other factors that are contributing to the organ shortage. These include:
- Disincentives for living organ donation (transplant-related medical expenses if not covered by the recipient’s insurance, loss of income while off work after the procedure, potential future insurability issues, etc.);
- Failure to engage the public in developing transplant policies (lack of input from donors and recipients that could result in better patient education, particularly about short- and long-term consequences of organ donation, such as insurability and health risks faced by living donors.)
- Low consent rates for deceased organ donation, driven partly by incorrect perceptions about the donation process, and partly by training gaps for medical personnel who request consent;
- The lack of transparency in disclosing and analyzing performance data for specific transplant centers and organ procurement organizations;
- A limited ability to accurately assess quality of donor organs based on currently available procurement testing. This may lead to discarding potentially transplantable organs.
This study showed that many people have questions and concerns about organ donation. Educating the public and improving transparency of the organ donation and transplantation process and performance are critical to narrowing the donor organ gap. Beyond that, the study concluded, reassessment of high-risk donor definitions, as well as the benchmarks for donor screening, are areas which could potentially improve the safety, quality and volume of organ procurement in the future.
_____
_____
Solution to organ shortage:
Organ shortage is the greatest challenge facing the field of organ transplantation today. Organ donation and transplant rates vary widely across the globe, but there remains an almost universal shortage of deceased donors. The unmet need for transplants has resulted in many systematic approaches to increase donor rates, but there have also been practices that have crossed the boundaries of legal and ethical acceptability. Recent years have seen intense interest from international political organizations, led by the World Health Organization, and professional bodies, led by The Transplantation Society. A variety of approaches have been implemented to expand the organ donor pool including live donation, a national effort to expand deceased donor donation, split organ donation, paired donor exchange, national sharing models and greater utilization of expanded criteria donors. Increased public awareness, improved efficiency of the donation process, greater expectations for transplantation, expansion of the living donor pool and the development of standardized donor management protocols have led to unprecedented rates of organ procurement and transplantation. Although live donors and donation after brain death account for the majority of organ donors, in the recent years there has been a growing interest in donors who have severe and irreversible brain injuries but do not meet the criteria for brain death. If the physician and family agree that the patient has no chance of recovery to a meaningful life, life support can be discontinued and the patient can be allowed to progress to circulatory arrest and then still donate organs (donation after circulatory death). Increasing utilization of marginal organs has been advocated to address the organ shortage. There has been extensive research on artificial or tissue-engineered organs and also on methods to preserve organs for longer periods of time.
_
Approaches to addressing this shortfall include:
- Donor registries and “primary consent” laws, to remove the burden of the donation decision from the legal next-of-kin. Illinois adopted a policy of “mandated choice” in 2006, which requires driver’s license registrants to answer the question “Do you want to be an organ donor?” Illinois has a registration rate of 60 percent compared to 38 percent nationally.
- Monetary incentives for signing up to be a donor. Some economists have advocated going as far as allowing the sale of organs. Gary Becker and Julio Jorge Elias argued in a recent paper that ‘monetary incentives would increase the supply of organs for transplant sufficiently to eliminate the very large queues in organ markets, and the suffering and deaths of many of those waiting, without increasing the total cost of transplant surgery by more than 12 percent.'” Iran allows the sale of kidneys, and has no waiting list. The primary argument against this proposal is a moral one; as the article notes, many find such a suggestion repugnant. As the National Kidney Foundation puts it, “Offering direct or indirect economic benefits in exchange for organ donation is inconsistent with our values as a society. Any attempt to assign a monetary value to the human body, or body parts, either arbitrarily, or through market forces, diminishes human dignity.”
- An opt-out system, in which a potential donor or his/her relatives must take specific action to be excluded from organ donation, rather than specific action to be included. This model is used in several European countries, such as Austria, which has a registration rate eight times that of Germany, which uses an opt-in system.
- Social incentive programs, wherein members sign a legal agreement to direct their organs first to other members who are on the transplant waiting list. One example of a private organization using this model is LifeSharers, which is free to join and whose members agree to sign a document giving preferred access to their organs. “The proposal [for an organ mutual insurance pool] can be easily summarized: An individual would receive priority for any needed transplant if that individual agrees that his or her organs will be available to other members of the insurance pool in the event of his or her death. … The main purpose [of this proposal] is to increase the supply of transplantable organs in order to save or improve more lives.”
_____
Extended criteria donors (ECD):
The persistent shortage of organ supplies is a major obstacle to carry out organ transplantation for the large number of people waiting on the list. Both the size of the candidate waiting list and the number of deaths on the waiting list are progressively increasing. The disparity between organ demand and organ supply has never been moderated. In order to decrease the mortality on the waiting list, transplant centers make every effort to increase the number of donors. Thus, utilization of extended criteria donors (ECD) has been suggested. In the early 2000s, the concept of extended criteria kidney donor was defined to older individuals with hypertension, diabetes, or renal dysfunction, who were expected to produce allografts at greater risk of graft loss than standard donors, albeit sufficiently adequate for transplantation. While the definition of extended criteria liver donor was characterized by individuals with advanced age, steatotic livers, donation after cardiac death (DCD), livers with seropositivity for hepatitis B virus (HBV) and hepatitis C virus (HCV). Besides, occult malignancies become a part of extended criteria donor factors. Using organs from donors with malignancy is not uncommon, and it has plays an important role in expanding the donor pool. Though this may carry risk of malignancy transmission, the risk of tumor transmission or donor related death is extremely small when compared with the benefits of organ transplantation.
_____
Alternate Listing Transplantation (ALT) strategy:
There is a critical scarcity of organs available for transplantation. Of an estimated 60,000 potential beneficiaries, fewer than 2,500 undergo cardiac transplantation annually. Given the significant disparities between the supply and demand for transplantable organs, strategies designed to offer transplantation to a greater number of candidates have the potential to provide substantial benefits. In order to achieve this goal, some centers have advocated for the adoption of Alternate Listing Transplantation (ALT). Under this strategy, high-risk (HR) candidates who fail to meet standard criteria for transplantation are considered for “marginal donor” (MD) organs—these organs do not meet standard donor criteria and would likely otherwise be left unused. Alternate listing, however, often means matching the highest risk recipients with poor quality donor organs; a phenomenon that may be associated with significant morbidity. A number of small studies have described outcomes using this strategy. These studies have largely found that ALT provides good long-term survival compared to that expected from end stage heart failure patients who do not undergo transplantation. A 2009 study found that pairing high-risk recipients with marginal donors is associated with greater morbidity and resource utilization compared with standard recipients and donors. Nevertheless, this strategy offers 5 years or more of additional survival to patients who otherwise would be expected to live 1 year or less. Therefore, ALT strategies appear to be a reasonable approach to extending the benefits of transplantation in the heart failure population.
_____
Organ donation from drug overdose deaths:
As the opioid epidemic has skyrocketed in the United States, a rise in the number of drug overdose deaths has contributed to a rise in organ transplants, made possible by overdose-death donors, across the country. A study published in the journal Annals of Internal Medicine reveals just how much of an increase there has been in the number of overdose-death donors, from being only 1.1% of all donors in 2000 to 13.4% in 2017. The study suggests that a rise in organ donations from drug overdose deaths could help America’s organ shortage — but it also shows that between 2000 and 2017, many organs from overdose-death donors were not used to save lives when they could have been. “The current epidemic of deaths from overdose is a tragedy. It would also be tragic to continue to underutilize life-saving transplants from donors,” said Dr. Christine Durand, assistant professor of medicine and oncology at Johns Hopkins University, who led the study. These donors require specialized testing for HIV and hepatitis as well as specialized consent for the transplant recipient. There is stigma related to this ‘increased infectious risk’ label. In reality, the ‘increased risk’ of HIV or hepatitis in these donors is very low. Patients who received transplants from these donors had excellent outcomes; patient survival and organ function were similar to cases when donors died due to trauma and similar or better than cases when the donor died due to medical causes of death, like heart attack or stroke. What was somewhat surprising was that, despite the good outcomes seen in transplant recipients, many organs donated after overdose death were discarded — that is, they were surgically recovered but then not used for transplant in any patient. During the course of the study, the researchers identified 1,665 kidneys, 501 livers, 117 hearts and 23 lungs from overdose-death donors that were recovered but discarded.
_____
Cryobanking:
The standard response to organ shortage is to call for more donors. But that’s not the answer. Far more organs are donated than used. Even the best preservation technologies can’t stop organs from deteriorating within hours after removal. And the whole transplant process takes time. First, tests are run to make sure that organs are immune compatible with potential recipients. Often, the donor’s family must give consent for the extraction. This takes more time. Then there are the logistical problems and costs of transport. So there may already be enough organs donated to save the lives of all those who need them. We just need to figure out a cost-efficient way to do it. We need to develop biotechnologies that allow organ banking.
In theory, organ banking could be done by freezing and then restoring organs as needed. Immune-matched organs could be supplied in a timely manner to patients at a reasonable cost.
Nature has shown us the way. Several types of fish that are native to polar waters produce antifreeze proteins (AFPs). AFPs protect cell structures and prevent harmful ice formation. This allows fish like the longhorn sculpin and the Antarctic eelpout to live in subzero temperatures. Molecules similar to AFPs could be used to preserve organs. But extraction of AFPs from these fish won’t work. It takes a ton of these rare fish to produce just a few grams of antifreeze protein. That means the species would be extinct if we had to rely on them. In December 2014, the US Department of Defense launched a program called “Organ Cryobanking for Transplants.” This was the first high-profile and well-funded effort to encourage this type of research. The move was applauded by scientists and other groups searching for viable organ banking. Then in 2015, the first Organ Banking Summit took place at Stanford University, NASA Research Park, and Lawrence Berkeley National Labs. The proceedings were published in the journal Cryobiology. This growing consensus on the need for cryobanking is having a positive impact. Perhaps most important, it gives private biotechs that have been working on the problem more credibility. A new nanoparticle technology warmed cryopreserved heart valves and blood vessels without damaging the tissues, according to a study published recently in the journal Science Translational Medicine. According to the researchers, this means that cryopreserving human hearts and kidneys in organ banks — and making them available for later use in patients — is finally within sight.
The ability to cryopreserve organs would result in numerous lives saved, better medical outcomes, lower costs, faster medical progress, and even better emergency transport systems, including UAV-based ambulances.
Organ Preservation Alliance says the ability to bank organs would confer a number of benefits:
- Better matches
- Fewer rejections
- Less immunosuppression
- More organs
- Lower costs
- Less disease transmission
- More lives saved in emergencies
- Better protection of fertility
From a technological perspective, we’re getting close to being able to pull this off. Already today, stem cells, sperm, eggs, and embryos are cryopreserved for long-term banking. Regular advances in ice blocker, cryoprotectants, and vitrification are now making it possible to preserve arteries, veins, heart valves, tracheas, cartilage, corneas, and even organ slices. Encouragingly, progress is being made with the preservation of rat hearts, pig and rodent livers — and even the remarkable cryopreservation and transplantation of a rabbit kidney.
_____
With Liver Donors in short supply, Cell Transplants offer New Options:
Called hepatocyte transplantation, the technique replaces approximately 10 percent of the liver with healthy cells from a deceased donor. The patient’s organ is not removed, decreasing recovery time, complications and cost. With fewer than 150 U.S. recipients so far, the approach is in its early days. If certain hurdles—such as the limited supply of cells and limited space in the patient’s liver—are overcome, hepatocyte transplantation may become an option for many liver disease sufferers. Some metabolic disorders, normally treated with whole-organ transplant, could be corrected with this less-intensive approach instead. For patients facing acute liver failure, hepatocyte transplantation could help their livers function until they recover. Some diseases for which liver transplantation would not be appropriate, such as amino acid disorders like phenylketonuria (PKU) and tyrosinemia, could also be treated with the new approach. And for those for whom no alternative exists and a transplant remains the only option, the procedure could also be used as a temporary measure, repeated as necessary until patients rose to the top of the waiting list—about 1,500 people die each year awaiting a transplant.
Hepatocytes are the liver’s main functional cells. In donated livers deemed unsuitable for transplantation the hepatocytes are usually still able to regenerate inside another liver. To extract them, the liver is chopped up and an enzyme called collagenase digests the fibrous matrix holding the cells together. White and red blood cells are removed, as are the bile duct cells. What remains are hepatocytes. Within 48 hours these fresh cells are infused into a patient through the portal vein, which carries blood to the liver, or through the umbilical vein at the navel, which flows into the portal vein. The new cells squeeze through spaces between the cells lining the portal vein and enter the liver where they meld with the patient’s own hepatocytes. “Then they just stay and live there,” says Ira Fox, a gastroenterologist pioneering the technique at the University of Pittsburgh. About one billion new cells can be introduced at each infusion.
______
Some technologies used for organ replacement:
| Technology | Supply | Feasibility now | Hurdles | Cost |
| Allotransplant | Limited | Yes | Supply and immunity | Moderate |
| ES cells | Unlimited | No | OF and immunity | Moderate or high |
| Cloning | Unlimited | No | OF and ? immunity | High |
| iPS cells | Unlimited | No | OF | High |
| Organogenesis | ? | No | Size, maturation, and function | High |
| In-vivo organogenesis | ? | No | Maturation and function | ? Moderate |
| Devices | Unlimited | Yes for heart | Toxicity and endurance | High |
| Xenotransplantation | Unlimited | Yes | Immunity | Low |
Cloning, cloning by nuclear transfer; ES cells, embryonic stem cells; iPS cells, induced pluripotent stem cells; OF, organ formation.
_____
_____
Tissue engineering and regenerative medicine:
Tissue engineering is the use of a combination of cells, engineering and materials methods, and suitable biochemical and physicochemical factors to improve or replace biological tissues. Tissue engineering involves the use of a tissue scaffold for the formation of new viable tissue for a medical purpose. Tissue engineering utilizes living cells as engineering materials. Examples include using living fibroblasts in skin replacement or repair, cartilage repaired with living chondrocytes, or other types of cells used in other ways. While it was once categorized as a sub-field of biomaterials, having grown in scope and importance it can be considered as a field in its own. The term regenerative medicine is often used synonymously with tissue engineering, although those involved in regenerative medicine place more emphasis on the use of stem cells or progenitor cells to produce tissues.
Examples:
- Bioartificial windpipe: The first procedure of regenerative medicine of an implantation of a “bioartificial” organ.
- In vitro meat: Edible artificial animal muscle tissue cultured in vitro.
- Bioartificial liver device: several research efforts have produced hepatic assist devices utilizing living hepatocytes.
- Artificial pancreas: research involves using islet cells to produce and regulate insulin, particularly in cases of diabetes.
- Artificial bladders: Anthony Atala (Wake Forest University) has successfully implanted artificially grown bladders into seven out of approximately 20 human test subjects as part of a long-term experiment.
- Cartilage: lab-grown tissue was successfully used to repair knee cartilage.
- Scaffold-free cartilage: Cartilage generated without the use of exogenous scaffold material. In this methodology, all material in the construct is cellular or material produced directly by the cells themselves.
- Doris Taylor’s heart in a jar
- Tissue-engineered airway
- Tissue-engineered vessels
- Artificial skin constructed from human skin cells embedded in a hydrogel, such as in the case of bioprinted constructs for battlefield burn repairs.
- Artificial bone marrow
- Artificial bone
- Laboratory-grown penis
- Oral mucosa tissue engineering
- Foreskin
_
Regenerative Medicine Applications in Organ Transplantation illustrates exactly how these two fields are coming together and can benefit one another. Recent ground-breaking achievements in regenerative medicine have received unprecedented coverage by the media, fuelling interest and enthusiasm in transplant clinicians and researchers. Regenerative medicine is changing the premise of solid organ transplantation, requiring transplantation investigators to become familiar with regenerative medicine investigations that can be extremely relevant to their work. Similarly, regenerative medicine investigators need to be aware of the needs of the transplant field to bring these two fields together for greater results.
_

Regenerative medicine is a branch of translational research in tissue engineering and molecular biology which deals with the “process of replacing, engineering or regenerating human cells, tissues or organs to restore or establish normal function”. This field holds the promise of engineering damaged tissues and organs by stimulating the body’s own repair mechanisms to functionally heal previously irreparable tissues or organs. Regenerative medicine also includes the possibility of growing tissues and organs in the laboratory and implanting them when the body cannot heal itself. If a regenerated organ’s cells would be derived from the patient’s own tissue or cells, this would potentially solve the problem of the shortage of organs available for donation, and the problem of organ transplant rejection. Some of the biomedical approaches within the field of regenerative medicine may involve the use of stem cells. Examples include the injection of stem cells or progenitor cells obtained through directed differentiation (cell therapies); the induction of regeneration by biologically active molecules administered alone or as a secretion by infused cells (immunomodulation therapy); and transplantation of in vitro grown organs and tissues (tissue engineering).
_____
Stem cell transplant for organ failure:
One subject that has resonated with the scientists, physicians, and the public has been the potential use of stem cells to treat disease, including organ failure. Some applications of stem cells have focused on repairing damaged organs such as the heart. Others have focused on generating new tissues and organs.
Four approaches for the generation of organ replacements from stem cells:
- First, mature tissue and even intact rodent organs have been generated in vitro by exploiting the natural ability of undifferentiated but committed fetal cells to form relatively differentiated and complex structures. Organogenesis in vitro can yield fully differentiated cells; however, tissues so generated lack blood vessels and do not approach the size of fetal organs, and achieving the size needed to replace an organ in a mature human would seem beyond the current or anticipated capabilities.
- Second, artificial devices and implantable organs have been proposed, and some constructed by seeding matrices, including de-cellularized organs, with mature cells or their precursors. Perhaps, the most advanced of these are the ‘bio-artificial liver devices’, which in experimental systems and clinical trials can exhibit discernable levels of function and clinical benefit; however, the devices have not been advanced to the point where they could be applied for the long-term treatment of hepatic failure. Nor have autologous stem cells been used toward this end. Thus, from a current perspective, an implantable, long-term liver replacement stands beyond the current technologies. Efforts are being made to use de-cellularized hearts and kidneys as a substrate for generating implantable cardiac and renal replacements. Seeding de-cellularized rodent heart with cardiac muscle cells and endothelial cells has yielded exciting levels of function in vitro, but long-term in-vivo testing and especially the development and testing of hearts repopulated using stem cells or their derivatives have not been reported and would seem remote, at least today.
- Third, undifferentiated fetal cells or partly differentiated stem cells or their derivatives might be implanted into the person to be treated, allowing in-vivo organogenesis to occur. Primitive cells from the animal fetuses have been advanced with some success; however, use of pluripotent stem cells in lieu of fetal cells has not been tested.
- Fourth, stem cells, of various types, might be engrafted into a developing xenogeneic fetus, allowing the microenvironment and growth factors of the fetus to coax the development of mature cells or of an organ, which can be transplanted into the person to be treated. Human hematopoietic stem cells engrafted in fetal swine generated a functional human immune system in the offspring and some mature human nephrons in the swine kidneys. However, whether this approach could be used to generate primordia in turn capable of generating whole human organs has not been tested and we fear the hurdles to doing so are considerable.
In sum, although many now envision the use of stem cells to generate organs or replace organ functions, no particular approach has emerged to accomplish that end.
_____
On the Horizon:
The need for organ transplantation may eventually be reduced by stem cell therapies. Scientists hope to repair or even replace damaged organs with new cells grown from adult or embryonic stem cells. In 2008, researchers at the University of Minnesota reported that they had built a beating heart in a laboratory with stem cells from neonatal and fetal rats. And scientists are undertaking clinical trials that attempt to repair the hearts of heart attack patients by injecting them with stem cells, and creating “heart patches” by combining stem-cells with other biomaterial. Patient-specific heart valves have been created by a method called “electrospinning” and implanted with apparent success. Another method called perfusion decellularization has enabled the creation of organ scaffolds into which individual-specific cells are seeded leading to structures that function very much like a heart, liver, vein, kidney, and bladder. In the near future, high resolution micro-imaging could create computer models of an individual’s ideal organ, which would dictate information to a bioprinter that would accurately place components like differentiated cells and growth factors, leading to a faithfully-reproduced fully-functional patient-specific organ. There is also increasing interest in using gene editing to create animals whose organs might be used in transplantation.
______
______
Organ engineering:
The concept is based upon the isolation of a three-dimensional, biological scaffold material, which has no cells in it. Lab technicians then take a patient’s own cells and use a technique developed in stem cell biology to plant these cells in the 3D scaffold, which take hold and grow a new organ. And since these cells belong to the patient, there’s no need for any immunosuppressant therapies. The fundamental concepts upon which this approach is based are already understood. Researchers know how to harvest a 3D scaffold for any organ. They can take a liver, lung, heart, or kidney and remove all of the cells from that organ so that you’re only left with the scaffold of the material that the cells resided upon. The scaffold material does not contribute to the rejection, yet it represents the perfect home for those types of cells. The second part of the process involves the reintroduction of cells. The researchers take a patient’s cells, such as a skin cell or a muscle cell, and convert it into a stem cell that can be driven along a particular line of differentiation. This way, a stem cell can be coaxed into becoming a liver cell, or a kidney cell, a heart cell, or whatever is required.
_
Stem Cell-Based Organ Transplants emerging as Alternative to Conventional Donations:
Engineered Trachea:
In Europe, an international team of surgeons and scientists has been transplanting stem cell-based tracheas since 2008. “We stripped the cells off the donor trachea, leaving just the extracellular matrix as a scaffold,” said Martin Birchall, MD, professor of laryngology at University College London Ear Institute. “Then we seeded the scaffold with stem cells taken from the patients’ own bone marrow.” The scaffold was bathed in a cocktail of hormones and growth factors to coax the growth of cell types associated with a normal trachea. In 2010, Dr. Birchall and colleagues, including pediatric cardiothoracic surgeon Martin Elliott, MD, performed the first pediatric, stem cell-based, tissue-engineered transplant, on a 10-year-old boy with congenital tracheal stenosis and pulmonary sling. He urgently needed a new trachea because the metal stent placed soon after his birth had eroded into his aorta, causing it to bleed. The patient, now 13, has a functioning airway. But in early 2011, the team treated a 36-year-old man with a rapidly growing laryngeal tumor. This patient didn’t have the luxury of waiting for a donor trachea. Instead, bioengineers at the University College London developed an artificial laryngotracheal scaffold from plastic. Then, just as with a cadaver trachea, it was seeded with stem cells and incubated in the growth medium, and within two days, the patient had his new airway. A few months later, a 30-year-old man, also with an inoperable tracheal tumor, underwent a similar operation. These two patients became the first humans to receive stem cell-based organ transplants. So far, the original patient is doing well, but the second patient has died, for reasons seemingly unrelated to the implant. In the meantime, two more patients, both from Russia, have received engineered tracheas.
______
Bioprinting:
Another hugely promising area in regenerative medicine is the process of 3D bioprinting. A leader in this area is Organovo, a San Diego-based medical lab and research company currently developing functional, three-dimensional human tissue via 3D bioprinting technology. The bioprinting process first involves the identification of the structural and compositional elements of the tissue that is to be printed and the creation of a viable design that can be utilized by the printer. Following this stage, a bioprocess protocol is developed to build the multi-cellular building blocks — which are called “bio-ink” — from the cells that will be used to generate the desired tissue. A bioprinter then dispenses the bio-ink in a layer-by-layer (or additive) manner. Sometimes a bio-inert hydrogel is used for support as tissues are constructed up vertically to achieve three-dimensionality, or as fillers to create channels or fill spaces like in normal tissue. In turn, Organovo is able to provide 3D mini liver assays that are architecturally and biologically (virtually) identical to human livers. This is a first-in-history capability that is allowing pharmaceutical companies to test liver toxicology at the very beginning of candidate molecule selection.
_
One person who’s looking to leverage the power of bioprinting is Dr. John Geibel, the vice chair of surgery and professor of surgery and cellular and molecular physiology at Yale School of Medicine. He says that bioprinting is poised “to change the way medicine is done in that, with the ability to print replacement vessels and eventually organs such as the liver, we will have the chance to save thousands of more individuals who are critically ill and on long wait lists for organ replacement.” Gobel says, the 3D liver assays can live for 42 days, but a heart for transplantation can currently be stored on ice for only 4-5 hours, and for lung tissue the cold ischemia time is around 4-6 hours.
_
Scientists have 3D printed artificial cornea using human cells, 2018 study:
The new technique described in the journal Experimental Eye Research, doesn’t completely eliminate a need for cornea donations — those are key for making the stem cell part of the recipe. But, using this technique, the donation goes a lot farther. Instead of replacing one damaged cornea with one healthy one, you could grow enough cells from one donated cornea to print 50 artificial ones. By using a simple 3D bio-printer, Professor of Tissue Engineering Che Connon and his team of scientists were able to combine healthy corneal stem cells with collagen and alginate (a type of sugar sometimes used in tissue regeneration) to create ‘bio-ink’ — a printable solution that enabled them to reproduce the shape of a human cornea in just 10 minutes. To figure out what exactly to print, the team also had to figure out the shape of a human cornea. So the researcher’s used a special camera to image a volunteer’s eyeball and create a 3D model of their cornea. Then, the team fed that template to a 3D printer, which squirted the bio-ink into a supportive bed of Jello to create the cornea. The result looks like a soft contact lens in a bath of goo. The artificial cornea will need to go through safety studies in animals.
_____
_____
Artificial organ transplantation:
Another alternative to organ transplantation would be creating artificial organs which could be used instead. An artificial organ is a synthetic man made device that is implanted into a human to replace an organ so that it can perform its job without needing constant maintenance such as recharging. Implied by definition, is that the device must not be continuously tethered to a stationary power supply or other stationary resources such as filters or chemical processing units. Thus, a dialysis machine, while a very successful and critically important life support device that almost completely replaces the duties of a kidney, is not an artificial organ. Significant progress has already been made in this field. Heart transplants can currently be given to those who urgently need it; however life cannot be reliably sustained after a period of about 18 months with this particular example. As well as artificial hearts; hands, eyes, lungs and livers and many more organs have been produced to varying degrees of success. Current research is going into making these transplants more efficient and less expensive. This is a high risk operation however, and the mortality rate for operations tends to be quite high. This leads to very difficult decisions having to be made by all those involved in the procedure including the patient. Clinical testing of new artificial organs is very difficult to carry out. It is only carried out on patients who have exhausted all over possible forms of therapy, some patients who are terminal and rarely, on violent convicts facing execution.
_____
_____
Xenotransplantation:
Xenotransplantation (xenos- from the Greek meaning “foreign”), is the transplantation of living cells, tissues or organs from one species to another. Such cells, tissues or organs are called xenografts or xenotransplants. Xenotransplantation is transplantation from one species to another; for example, from a pig to a human. The term covers transplantation of solid organs (such as kidney or heart), tissues (such as skin) or clusters of specialised cells (such as brain cells or the pancreatic cells that produce insulin). Xenotransplantation can also involve the infusion or transplantation of body fluids, tissues or cells that have been in contact with the tissues or cells of another species outside the recipient’s body. For example, a person might be treated for liver failure by having their blood passed through an artificial device containing pig liver cells. Some nonliving animal devices, such as pig heart valves, have been used in humans for many years. Xenotransplants differ from these devices in that they are alive and can perform the same functions as the organ, tissue or cells that they replace. Xenotransplantation of human tumor cells into immunocompromised mice is a research technique frequently used in pre-clinical oncology research. Human xenotransplantation offers a potential treatment for end-stage organ failure, a significant health problem in parts of the industrialized world. It also raises many novel medical, legal and ethical issues. A continuing concern is that many animals, such as pigs, have a shorter lifespan than humans, meaning that their tissues age at a quicker rate. Disease transmission (xenozoonosis) and permanent alteration to the genetic code of animals are also causes for concern. A few successful cases of xenotransplantation are published.
_
Xenotransplantation is a method that involves taking the tissues, organs and other parts of the body from animals and then transplanting them into other animals, human beings included. The concept of this procedure has been sparking a lot of heated debates around the world, as many people feel uncomfortable thinking that pig parts would be transplanted into humans. Also, it has created a moral dilemma based on religious beliefs, the disposition to have an animal part in a person’s body and the psychological issues that some individuals would have to overcome before they would get used to the idea of such a procedure. While there has not been great success with this method of organ transplantation, researchers and scientists did manage to successfully replace parts, such as skin and heart valves. In most cases, organ transplants were not really able to provide a viable solution, as the immunosuppressant drugs that were used to prevent the body from attacking a new organ have led to infections that are potentially fatal in their own right. However, the continued research on finding better ways to use animal tissues and organs in human subjects has also provided great opportunities.
_
Xenotransplantation takes a number of forms:
- Transplantation of solid animal organs (such as hearts, kidneys, livers);
- Cell therapies, such as the transplantation of pig neural cells and pig pancreatic islet cells;
- The use of viable animal cells as part of a medical device, such as an extra-corporeal liver;
- The use of animal cells in gene therapies.
_
Transplantation between members of the same species is known as allotransplantation, and in humans this is a very successful way to treat a variety of illnesses. However, very few human tissues and organs are available for transplantation, so that many patients who could benefit from a transplant wait in vain for a suitable donor. Transplant specialists are therefore considering animals as a possible source of organs and tissues for human transplantation. The greatest benefit of xenotransplantation would be a potentially unlimited supply of cells, tissues and organs for use in humans. Recent advances in technology have increased the possibility of successful xenotransplantation and stimulated research in this area. For example, genetic engineering has allowed human genes to be inserted into pigs so that their cells, tissues and organs are less likely to be rejected when transplanted into humans. Another possibility is that xenotransplantation could be used to ‘buy time’ while potential transplant patients wait for a suitable donor. There have been promising results from overseas trials in which isolated pig liver cells contained in a bioreactor were used to treat acute liver failure.
_
Donor-recipient combinations can be classified, as was initially done by Calne, into ‘discordant’ (where transplant between species results in a rapid, hyperacute rejection) or ‘concordant’ (where rejection occurs at a pace similar to that of allotransplantation). We know that this difference is essentially due to the presence or absence of preformed antibodies. Blood transfusions from animals to man were performed in England and France from the early seventeenth century. These were the first clinical attempts at xenotransplantation. Solid organ transplants, attempted in the 20th century, had one or two successes, again mainly in concordant transplants. Reemtsma and colleagues reported patients surviving up to nine months after kidney transplants from a chimpanzee. They also showed that acute cellular rejection could be reversed by high doses of steroids. By contrast, organ transplants from non-primates have had little success, graft survival being measured in hours or minutes. With cells the picture is somewhat more promising: pig hepatocytes have been incorporated into extracorporeal liver assist devices, and non-primate tissue has also been used with varying success in treatment of diabetes and parkinsonism. Although nonhuman primates are phylogenetically closer than other species to humans, for a number of reasons they are not considered to be a suitable source of organs for clinical xenotransplantation. The potentially high risk of cross species transmission of infection to humans, difficulties in breeding, organ size disparities and other impracticalities, as well as ethical issues have largely excluded them from further consideration. The pig is now the preferred source. Pigs are currently thought to be the best candidates for organ donation. The risk of cross-species disease transmission is decreased because of their increased phylogenetic distance from humans. They are readily available, their organs are anatomically comparable in size, and new infectious agents are less likely since they have been in close contact with humans through domestication for many generations. Current experiments in xenotransplantation most often use pigs as the donor, and baboons as human models.
__
Extensive research is required to determine whether animal organs can replace the physiological functions of human organs. Many issues include:
- Size – Differences in organ size limit the range of potential recipients of xenotransplants.
- Longevity – The lifespan of most pigs is roughly 15 years, currently it is unknown whether or not a xenograft may be able to last longer than that.
- Hormone and protein differences – Some proteins will be molecularly incompatible, which could cause malfunction of important regulatory processes. These differences also make the prospect of hepatic xenotransplantation less promising, since the liver plays an important role in the production of so many proteins.
- Environment – For example, pig hearts work in a different anatomical site and under different hydrostatic pressure than in humans.
- Temperature – The body temperature of pigs is 39 °C (2 °C above the average human body temperature). Implications of this difference, if any, on the activity of important enzymes are currently unknown.
_
The advantages and disadvantages of the pig vs. baboon as a potential source of organs and cells for humans:
| Pig | Baboon | |
| Availability | Unlimited | Limited |
| Breeding potential | Good | Poor |
| Period to reproductive maturity | 4–8 months | 3–5 years |
| Length of pregnancy | 114 ± 2 days | 173–193 days |
| Number of offspring | 5–12 | 1–2 |
| Growth | Rapid (adult human size within 6 months) | Slow (9 years to reach maximum size) |
| Size of adult organs | Adequate | Inadequate∗ |
| Cost of maintenance | Significantly lower | High |
| Anatomical similarity to humans | Moderately close | Close |
| Physiological similarity to humans | Moderately close | Close |
| Relationship of immune system to humans | Distant | Close |
| Knowledge of tissue typing | Considerable (in selected herds) | Limited |
| Necessity for blood type compatibility with humans | Probably unimportant | Important |
| Experience with genetic engineering | Considerable | None |
| Risk of transfer of infection (xenozoonosis) | Low | High |
| Availability of specific pathogen-free animals | Yes | Yes |
| Public opinion | More in favor | Mixed |
__
Why use pigs?
Pigs are considered the most suitable species as a source of material for xenotransplantation for several reasons:
- they reproduce quickly and have large litters;
- their organs are similar in size to those of humans;
- they are easy to rear in conditions free of particular pathogens (disease-causing organisms);
- the risk that they will carry pathogens that can infect humans is smaller than with nonhuman primates (apes and monkeys); and
- they can be genetically manipulated to reduce the risk of rejection.
__
Obstacles to xenotransplantation
Aside from ethical considerations, there are three main obstacles to successful xenotransplant: physiological, microbiological, and immunological.
- Porcine and human physiology differs in a number of important aspects. There are differences in organ perfusion pressures and core temperatures (the latter being 39°C in the pig). There are also differences in structure and activity of a variety of proteins, particularly those involved in the clotting and complement cascades and cell regulation.
- The second concern relates to zoonotic infection, particularly from porcine endogenous retroviruses (PERVs). Several PERVs have been identified in the genome of pigs, some of which have been shown to infect human cells in culture. The significance of these in clinical transplantation in an immunosuppressed recipient is unknown, but a cause for concern.
- The third challenge is immunological. Genetic manipulation of pig endothelium to express human complement regulatory proteins overcomes the immediate threat of antibody-mediated hyperacute rejection response that would otherwise be a consequence of humans having preformed natural antibodies to porcine antigens. However, the threat of subsequent cell-mediated rejection has proven more resistant to genetic manipulation, with the cellular response to pig antigens that are indirectly presented on human MHC molecules being particularly aggressive. It would appear that xenotransplantation is still some years away from clinical practice.
_____
Immunologic barriers to xenotransplantation:
To date no xenotransplantation trials have been entirely successful due to the many obstacles arising from the response of the recipient’s immune system. This response, which is generally more extreme than in allotransplantations, ultimately results in rejection of the xenograft, and can in some cases result in the immediate death of the recipient. There are several types of rejection organ xenografts are faced with, these include:
- Hyperacute rejection
- Acute vascular rejection
- Cellular rejection
- Chronic rejection
_
Hyperacute rejection:
This rapid and violent type of rejection occurs within minutes to hours from the time of the transplant. It is mediated by the binding of XNAs (xenoreactive natural antibodies) to the donor endothelium, causing activation of the human complement system, which results in endothelial damage, inflammation, thrombosis and necrosis of the transplant. XNAs are first produced and begin circulating in the blood in neonates, after colonization of the bowel by bacteria with galactose moieties on their cell walls. Most of these antibodies are the IgM class, but also include IgG, and IgA. The epitope XNAs target is an α-linked galactose moiety, Gal-α-1,3Gal (also called the α-Gal epitope), produced by the enzyme α-galactosyl transferase. Most non-primates contain this enzyme thus, this epitope is present on the organ epithelium and is perceived as a foreign antigen by primates, which lack the galactosyl transferase enzyme. In pig to primate xenotransplantation, XNAs recognize porcine glycoproteins of the integrin family. The binding of XNAs initiate complement activation through the classical complement pathway. Complement activation causes a cascade of events leading to: destruction of endothelial cells, platelet degranulation, inflammation, coagulation, fibrin deposition, and hemorrhage. The end result is thrombosis and necrosis of the xenograft.
Overcoming hyperacute rejection:
Since hyperacute rejection presents such a barrier to the success of xenografts, several strategies to overcome it are under investigation:
–Interruption of the complement cascade
The recipient’s complement cascade can be inhibited through the use of cobra venom factor (which depletes C3), soluble complement receptor type 1, anti-C5 antibodies, or C1 inhibitor (C1-INH). Disadvantages of this approach include the toxicity of cobra venom factor, and most importantly these treatments would deprive the individual of a functional complement system.
–Plasmapheresis, on humans to remove 1,3 galactosyltransferase, reduces the risk of activation of effector cells such as CTL (CD8 T cells), complement pathway activation and delayed type hypersensitivity (DTH).
–Transgenic organs (Genetically engineered pigs)
- 1,3 galactosyl transferase gene knockouts – These pigs don’t contain the gene that codes for the enzyme responsible for expression of the immunogeneic gal-α-1,3Gal moiety (the α-Gal epitope).
- Increased expression of H-transferase (α 1,2 fucosyltransferase), an enzyme that competes with galactosyl transferase. Experiments have shown this reduces α-Gal expression by 70%.
- Expression of human complement regulators (CD55, CD46, and CD59) to inhibit the complement cascade.
_
Acute vascular rejection:
Also known as delayed xenoactive rejection, this type of rejection occurs in discordant xenografts within 2 to 3 days, if hyperacute rejection is prevented. The process is much more complex than hyperacute rejection and is currently not completely understood. Acute vascular rejection requires de novo protein synthesis and is driven by interactions between the graft endothelial cells and host antibodies (XNAs), macrophages, and platelets. The response is characterized by an inflammatory infiltrate of mostly macrophages and natural killer cells (with small numbers of T cells), intravascular thrombosis, and fibrinoid necrosis of vessel walls.
Overcoming acute vascular rejection:
Due to its complexity, the use of immunosuppressive drugs along with a wide array of approaches are necessary to prevent acute vascular rejection, and include:
- Administering a synthetic thrombin inhibitor to modulate thrombogenesis
- Depletion of anti-galactose antibodies (XNAs) by techniques such as immunoadsorption, to prevent endothelial cell activation
- Inhibiting activation of macrophages (stimulated by CD4+ T cells) and NK cells (stimulated by the release of Il-2). Thus, the role of MHC molecules and T cell responses in activation would have to be reassessed for each species combo.
_
Accommodation:
If hyperacute and acute vascular rejection are avoided accommodation is possible, which is the survival of the xenograft despite the presence of circulating XNAs. The graft is given a break from humoral rejection when the complement cascade is interrupted, circulating antibodies are removed, or their function is changed, or there is a change in the expression of surface antigens on the graft. This allows the xenograft to up-regulate and express protective genes, which aid in resistance to injury, such as heme oxygenase-1 (an enzyme that catalyzes the degradation of heme).
_
Cellular rejection:
Rejection of the xenograft in hyperactute and acute vascular rejection is due to the response of the humoral immune system, since the response is elicited by the XNAs. Cellular rejection is based on cellular immunity, and is mediated by:
- Natural killer cells, which accumulate in and damage the xenograft; and
- T-lymphocytes – which are activated by MHC molecules through both direct and indirect xenorecognition.
In direct xenorecognition, antigen presenting cells from the xenograft present peptides to recipient CD4+ T cells via xenogeneic MHC class II molecules, resulting in the production of interleukin 2 (IL-2). Indirect xenorecognition involves the presentation of antigens from the xenograft by recipient antigen presenting cells to CD4+ T cells. Antigens of phagocytosed graft cells can also be presented by the host’s class I MHC molecules to CD8+ T cells.
The strength of cellular rejection in xenografts remains uncertain, however it is expected to be stronger than in allografts due to differences in peptides among different animals. This leads to more antigens potentially recognized as foreign, thus eliciting a greater indirect xenogenic response.
Overcoming cellular rejection:
A proposed strategy to avoid cellular rejection is to induce donor non-responsiveness using hematopoietic chimerism. Donor stem cells are introduced into the bone marrow of the recipient, where they coexist with the recipient’s stem cells. The bone marrow stem cells give rise to cells of all hematopoietic lineages, through the process of hematopoiesis. Lymphoid progenitor cells are created by this process and move to the thymus where negative selection eliminates T cells found to be reactive to self. The existence of donor stem cells in the recipient’s bone marrow causes donor reactive T cells to be considered self and undergo apoptosis.
_
Chronic rejection:
Chronic rejection is slow and progressive, and usually occurs in transplants that survive the initial rejection phases. Scientists are still unclear how chronic rejection exactly works, research in this area is difficult since xenografts rarely survive past the initial acute rejection phases. Nonetheless, it is known that XNAs and the complement system are not primarily involved. Fibrosis in the xenograft occurs as a result of immune reactions, cytokines (which stimulate fibroblasts), or healing (following cellular necrosis in acute rejection). Perhaps the major cause of chronic rejection is arteriosclerosis. Lymphocytes, which were previously activated by antigens in the vessel wall of the graft, activate macrophages to secrete smooth muscle growth factors. This results in a build-up of smooth muscle cells on the vessel walls, causing the hardening and narrowing of vessels within the graft. Chronic rejection leads to pathologic changes of the organ, and is why transplants must be replaced after so many years. It is also anticipated that chronic rejection will be more aggressive in xenotransplants as opposed to allotransplants.
_
Dysregulated coagulation:
Successful efforts have been made to create knockout mice without α1,3GT; the resulting reduction in the highly immunogenic αGal epitope has resulted in the reduction of the occurrence of hyperacute rejection, but has not eliminated other barriers to xenotransplantation such as dysregulated coagulation, also known as coagulopathy. Different organ xenotransplants result in different responses in clotting. For example, kidney transplants result in a higher degree of coagulopathy, or impaired clotting, than cardiac transplants, whereas liver xenografts result in severe thrombocytopenia, causing recipient death within a few days due to bleeding. An alternate clotting disorder, thrombosis, may be initiated by preexisting antibodies that affect the protein C anticoagulant system. Due to this effect, porcine donors must be extensively screened before transplantation. Studies have also shown that some porcine transplant cells are able to induce human tissue factor expression, thus stimulating platelet and monocyte aggregation around the xenotransplanted organ, causing severe clotting. Additionally, spontaneous platelet accumulation may be caused by contact with pig von Willebrand factor. Just as the α1,3G epitope is a major problem in xenotransplantation, so too is dysregulated coagulation a cause of concern. Transgenic pigs that can control for variable coagulant activity based on the specific organ transplanted would make xenotransplantation a more readily available solution.
_____
Current results of experimental pig organ or cell xenotransplantation:
The experimental results of cell xenotransplantation, e.g., islet or neuronal cells, are currently significantly better than those of pig organ xenotransplantation. For example, pig islets have continued to function effectively in immunosuppressed nonhuman primates for periods of more than a year. Indeed, a clinical trial of encapsulated pig islet transplantation is under way in diabetic patients in New Zealand. There are an estimated 8 million patients in the US with a neurogenerative disease, such as Parkinson’s disease. Human embryonic neural precursor cells can restore local motor activity in patients with Parkinson’s disease, but the use of human embryos is largely precluded on ethical grounds or on logistic grounds as too few become available. Genetically engineered pig embryos might provide an alternative source. Indeed, a European group has reported encouraging improvement for >1 year in locomotor function in monkeys with a Parkinson-like condition after the transplantation of genetically modified pig dopamine-producing cells into the brain. There is also a great need for corneas, particularly in Asia and Africa; for example, it is estimated that 4 million patients need corneal transplantation in China alone. Experimental corneal xenotransplantation has made significant progress in recent years; pig lamellar grafts have survived in monkeys for periods of more than 1 year, with the recipient receiving only corticosteroid injections into the eyes. Partly because the risk to the recipient would be small, it is likely that corneas will be the first xenotransplants to be carried out as a clinical trial, perhaps followed soon after by neuronal cell or islet cell transplantation. With regard to pig organ xenotransplantation in nonhuman primates, researchers have been able to achieve pig heterotopic cardiac graft survival up to 8 months (i.e., non–life-supporting grafts in which the graft is placed in the abdomen and, by being supplied with recipient blood, beats, thus allowing monitoring for rejection) and life-supporting pig kidney survival up to almost 3 months. Transplantation of pig livers and lungs in nonhuman primates has been significantly less successful, with grafts functioning for only days. Pig hearts and livers may initially be used as a bridge while the patient is awaiting a human graft; this will give us experience with organ xenografts in humans. Because dialysis maintains life for a number of years in many patients with renal failure, clinical pig kidney transplantation will probably be delayed.
_____
Genetically engineered pigs:
Most of the advances that have been made in this field have resulted from the introduction of genetically engineered pigs. The most significant advances to date have been the production of pigs expressing a human complement-regulatory protein (e.g., human decay-accelerating factor [CD55], membrane cofactor protein [CD46] or CD59) and pigs in which the gene for α1,3-galactosyltransferase has been knocked out (α1,3-galactosyltransferase gene-knockout [GTKO] pigs). The presence of a complement-regulatory protein on the surface of vascular endothelial cells in the pig largely protects the graft from hyperacute rejection. Of interest is the suggestion that overexpression of a pig complement-regulatory protein might be as effective as the expression of a human complement-regulatory protein in protecting the pig cell from lysis, although this theory has never been tested in an in vivo model. The gene for α1,3-galactosyltransferase enables this enzyme to add Gal α1,3Gal (Gal) oligosaccharides to various underlying glycoproteins and glycolipids in the pig. Gal is the major target for human and nonhuman primate antipig antibodies, and its deletion from pigs has greatly reduced the incidence of hyperacute rejection of pig grafts in nonhuman primates. GTKO pigs additionally transgenic for a human complement-regulatory protein provide increased benefit over each modification alone. IgM, IgG and complement deposition in grafts is absent or less marked, and innate cellular infiltration has also been minimized. Genetically engineered pig hearts placed heterotopically in baboons have functioned for periods of 3–6 months, life-supporting kidneys for periods approaching 3 months, livers for a matter of days, and lungs for a matter of hours. With gene-editing tools such as CRISPR, scientists can now eliminate immune-provoking sugars from the surface of pig cells, introduce human genes that regulate blood coagulation to prevent dangerous clots, and snip out viral sequences that some fear could infect a human host.
_____
Risks of xenotransplantation:
- Xenograft Rejection:
The key obstacle to using pig organs and cells for transplantation in humans is the strong immune response by porcine antigens (vide supra).
- Xenozoonosis:
Xenozoonosis, also known as zoonosis or xenosis, is the transmission of infectious agents between species via xenograft. Animal to human infection is normally rare, but has occurred in the past. An example of such is the avian influenza, when an influenza A virus was passed from birds to humans. Xenotransplantation may increase the chance of disease transmission for 3 reasons:
- Implantation breaches the physical barrier that normally helps to prevent disease transmission,
- The recipient of the transplant will be severely immunosuppressed; and
- Human complement regulators (CD46, CD55, and CD59) expressed in transgenic pigs have been shown to serve as virus receptors, and may also help to protect viruses from attack by the complement system.
Examples of viruses carried by pigs include porcine herpes virus, rotavirus, parvovirus, and circovirus. Porcine herpes viruses and rotaviruses can be eliminated from the donor pool by screening, however others (such as parvovirus and circovirus) may contaminate food and footwear then re-infect the herd. Thus, pigs to be used as organ donors must be housed under strict regulations and screened regularly for microbes and pathogens. Unknown viruses, as well as those not harmful in the animal, may also pose risks. Of particular concern are PERVs (porcine endogenous retroviruses), vertically transmitted microbes that embed in swine genomes. The risks with xenosis are twofold, as not only could the individual become infected, but a novel infection could initiate an epidemic in the human population. Because of this risk, the FDA has suggested any recipients of xenotransplants shall be closely monitored for the remainder of their life, and quarantined if they show signs of xenosis. Risks can be minimized by using animals from strictly controlled herds such as pigs that are grown in test laboratories or government farms. Many such agents can be eliminated from the pig herd through scrupulous husbandry methods. Such methods include the sterilization of both feed and drinking water and the elimination of all mammalian protein from the feed to prevent prion infection. Unfortunately, this does not eliminate the risk of transmitting viruses whose DNA is integrated into the nucleus of transplanted cells, such as porcine endogenous retroviruses (PERVs).
- There are ethical concerns:
Opposition to xenotransplantation has been widespread since the procedure was first attempted. Animal rights groups in particular have been vocal about the killing of animals to harvest their organs for use in humans. Jewish and Islamic communities prohibit the consumption of pig. Although there have been no major objections from major religions over the use of genetically modified pig organs for organ transplants, there have been objections from those with certain religious beliefs.
____
Regulation of xenotransplantation:
In the United States, the regulatory responsibility lies with the Food and Drug Administration (FDA) which has updated its “Public Health Service Guidelines on Infectious Disease Issues in Xenotransplantation” that were first released in September 1996. Clinical trials involving xenotransplantation have been approved by the FDA. In Great Britain, a moratorium on clinical trials was introduced in January 1997, but clinical trial applications may now be submitted for review to the United Kingdom Xenotransplantation Interim Regulatory Authority (UKXIRA). UKXIRA was established in May 1997, to advise the UK Health departments on actions necessary to regulate xenotransplantation and to advise on the acceptability of clinical trial applications. UKXIRA has not approved any clinical trials to date. The World Health Organization, in its efforts to foster international consensus on issues related to human health, hosted a consultation with international experts and published guidelines in 1998 on preventing and managing infectious diseases associated with xenotransplantation. In January 1999, the Council of Europe’s Parliamentary Assembly called for a moratorium on xenotransplantation until this new technology is evaluated and guidelines are established and agreed. The Assembly also asked the Council of Europe Public Health and Bioethics Committees to work hand in hand with the World Health Organisation on a strategy which balances ethical, medical, scientific, legal, social and public health issues before human clinical trials continue.
_____
_____
Head transplant:
A head transplant is an experimental surgical operation involving the grafting of one organism’s head onto the body of another; in many experiments the recipient’s head was not removed but in others it has been. Experimentation in animals began in the early 1900s. As of 2018, no durable success had been achieved. Scientists have long dreamed of cutting someone’s head off and putting it onto someone else’s body. Yes, there are altruistic reasons for doing this—ideally doctors could one day take the head of someone who’s paralyzed, has lost limbs, or has other serious medical issues, and graft it onto a healthy body. While no one’s successfully transplanted a head, there’s a long, gruesome history of making attempts with dogs. As early as 1908, French organ transplant pioneer Alexis Carrel and American physiologist Charles Claude Guthrie attempted to graft a dog’s head onto a second dog (with the second dog’s head still intact). The grafted head initially showed some basic reflexes, but died soon after and the intact dog was put down. Transplanting heads is not easy. There are three main technical challenges. As with any organ transplant, managing the immune response to avoid transplant rejection is necessary. Also, the brain is highly dependent on continuous flow of blood to provide oxygen and nutrients and remove waste products, with damage setting in quickly at normal temperatures when blood flow is cut off. Finally, managing the nervous systems in both the body and the head is essential, in several ways. The autonomic nervous system controls essential functions like breathing and the heart beating and is governed largely by the brain stem; if the recipient body’s head is removed this can no longer function. Additionally each nerve coming out of the head via the spinal cord needs to be connected to the putatively corresponding nerve in the recipient body’s spinal cord in order for the brain to control movement and receive sensory information. Finally, the risk of systematic neuropathic pain is high and as of 2017 had largely been unaddressed in research.
_
Brain transplant:
A brain transplant is a procedure in which the brain of one organism is transplanted into the body of another. It is a procedure distinct from head transplantation, which involves transferring the entire head to a new body, as opposed to the brain only. Theoretically, a person with advanced organ failure could be given a new and functional body while keeping their own personality, memories, and consciousness through such a procedure. One of the most significant barriers to the procedure is the inability of nerve tissue to heal properly; scarred nerve tissue does not transmit signals well (this is why a spinal cord injury is so devastating). Research at the Wistar Institute of the University of Pennsylvania involving tissue-regenerating mice (known as MRL mice) may provide pointers for further research as to how to regenerate nerves without scarring. It is possible that a completely clean cut will not generate scarred tissue. The brain was thought to be an immunologically privileged organ, so rejection would not be a problem. When other organs are transplanted, aggressive rejection can occur; this is a major difficulty with kidney and liver transplants. Immune cells of the CNS contribute to the maintenance of neurogenesis and spatial learning abilities in adulthood, so the transplanted brain would not be unhindered from the transplant. No human brain transplant has ever been conducted. Neurosurgeon Robert J. White, has grafted the head of a monkey onto the headless body of another monkey. EEG readings showed the brain was later functioning normally. It was thought to prove that the brain was an immunologically privileged organ, as the host’s immune system did not attack it at first, but immunorejection caused the monkey to die after nine days. Brain transplants and similar concepts have also been explored in various forms of science fiction.
_____
_____
Myths regarding organ donation and transplantation:
_
- Myth: Organ and tissue donation mutilates the body.
Fact: Donated organs are removed surgically, which doesn’t disfigure the body. The donor’s body is clothed for cremation/burial, so there are no visible signs of donation. After eye donation, an artificial eye is inserted, the eyelids are closed, and no one can notice any difference. After bone donation, a rod is inserted where the bone has been removed. With skin donation, a very thin layer of skin similar to a sunburn peel is taken from the donor’s back.
_
- Myth: Anyone can be an organ donor.
Fact: Anyone cannot be organ donor but anyone can register as a prospective donor. Surgeons recover organs from patients with beating hearts or just stopped beating before them. Surgeons don’t recover vital organs from donors who are completely dead and whose hearts have stopped beating as such organs have suffered ischemic damage. Some diseases rule out donation including active cancer, active HIV or active infection. For a person with a history of hepatitis, more information would be required at the time of death. Persons with Hepatitis C may still donate organs to a patient who also has Hepatitis C. Since organs from donors whose heart has stopped (non-heart beating) is not be suitable for transplantation, only 0.3 to 1% of prospective donors finally donate vital organs. Donation of eyes, bone and skin is possible from non-heart beating donors.
_
- Myth: I’m under age 18. I’m too young to make this decision.
Fact: That’s true, in a legal sense. But your parents can authorize this decision. You can express to your parents your wish to donate, and your parents can give their consent knowing that it’s what you wanted. Children, too, are in need of organ transplants, and they usually need organs smaller than those an adult can provide.
_
- Myth: If the ICU doctors know I’m an organ donor, they won’t work hard to save me.
Fact: If you are admitted in a hospital – sick or injured, the priority is to save your life. Organ donation can only be considered after brain death occurs. Moreover, the medical team treating you is distinct from the transplant team.
_
- Myth: Old people cannot donate organs.
Fact: There’s no defined cut-off age. Organs have been successfully transplanted from donors in their 70s and 80s! However, in a donor above the age of 70 years, the matter needs to be reviewed by the authorities concerned before organ donation is permitted. At the time of death, only the doctors can decide whether the organs are suitable for transplantation.
_
- Myth: Having “organ donor” noted on the driver’s licence or carrying a donor card is all that’s required to become a donor. I don’t need to tell my family I want to be a donor because it is written in my will.
Fact: Signed donor card and a driver’s licence with an “organ donor” statement are an expression of your desire to be a donor. Organ donation is usually discussed with family members prior to the donation. To ensure your family understands and respects your wishes, it’s important that you tell them about your decision to donate organ to save someone’s life. By the time your will is read, it will be too late to recover your organs. Informing your family in advance is the best way to ensure your wishes are carried out.
_
- Myth: Organ donation will not delays funeral arrangements.
Fact: Yes, there is a possibility of funeral delay. However, given the altruistic nature of this donation, families usually accept this and take it as part of the process of donation.
_
- Myth: I’d like to donate one of my kidneys now, but I wouldn’t be allowed to do that unless one of my family members is in need.
Fact: While that used to be the case, it isn’t any longer. Whether it’s a distant family member, friend or complete stranger you want to help, you can donate a kidney through certain transplant centers. If you decide to become a living donor, you will undergo extensive questioning to ensure that you are aware of the risks and that your decision to donate isn’t based on financial gain. You will also undergo testing to determine if your kidneys are in good shape and whether you can live a healthy life with just one kidney.
_
- Myth: I cannot choose which organs I want to donate.
Fact: On your donor card, you can list which organs and tissues you’re willing to donate.
_____
_____
Moral of the story:
_
- According to WHO, the term “human organ” is understood to include organs and tissues but does not relate to human reproduction, and accordingly does not extend to reproductive tissues, namely ova, sperm, ovaries, testicles or embryos, nor is it intended to deal with blood or blood constituents for transfusion purposes.
_
- Organ donation is when a person allows healthy organ/tissue of theirs to be removed legally, either by consent while the donor is alive or after death with the assent of the next of kin, to be transplanted into another person. Organ transplantation is the moving of a whole or partial organ from one body to another (or from a donor site on the patient’s own body), for the purpose of replacing the recipient’s damaged or failing organ with a working one from the donor site. A transplant (graft) is an organ, tissue or a group of cells removed from one person (the donor) and surgically transplanted into another person (the recipient or host) or moved from one site to another site in the same person. Common transplantations include: kidneys, heart, liver, pancreas, intestines, lungs, bones, bone marrow, skin, and corneas.
_
- Patients are generally considered for listing for a transplant if they have a better than 50% chance of surviving 5 year after transplant. Organ transplantation is the best therapy for terminal and irreversible organ failure. Transplantation has given many a new lease on life and, to many more, an extension that would have otherwise been impossible. In general, organ transplantation saves lives, prolongs survival, and increases the quality of life. There is a significant difference in the median survival time between patients on the waiting list and transplant recipients. A study found that getting an organ transplant could add four or more years to recipient’s life. A pancreas transplant alone, an often controversial option, confers a median survival time of 13.6 years (compared with 8 years in patients on the waiting list). A kidney transplant doubles median survival time compared to staying on kidney dialysis treatment.
_
- About 120,000 organs are transplanted annually worldwide but the annual number of organ transplants represents less than 10% of the global needs. Approximately 500,000 people die every year in India due to unavailability of organs. Almost 96,000 people die each year in the U.S. waiting for a new kidney.
_
- Many see organ donation as a sensible, practical thing to do after death. Within few months after burial, the bacteria will eat all organs except bones. Within few hours of cremation, all organs become smoke and ashes. Instead of feeding our-self to bacteria or becoming smoke & ashes, why shouldn’t we donate organs to someone who lives?
_
- The donated organ may be from a deceased donor (previously referred to as cadaveric or non-living donor), a living donor, or an animal. In some cases an artificial organ is used. Cadaveric organ donation involves removing organs from a recently deceased donor (brain dead, or dead via circulatory death). Most deceased organ donation occurs after brain death, known as donation after brain death (DBD). A beating heart cadaver is kept alive in order to keep its organs from decaying before they can be transplanted. Although brain-dead (or “heart beating”) donors are considered to be dead, the donor’s heart continues to pump and maintain the circulation. This makes it possible for surgeons to start operating while the organs are still being perfused (supplied with blood). Donation after cardio-circulatory Death (DCD) involves donation from a patient with a severe brain injury who does not meet the criteria for brain death but who has no chance of recovery and is removed from life-sustaining therapy with the consent of his or her family. Accordingly death is declared 5 minutes after the heart stops beating. In these cases, the organs must be removed within a few minutes of the heart stopping to prevent them being damaged by a lack of oxygenated blood. Organs from circulatory-death donors have inferior outcomes compared to organs from a brain-dead donor. Living organ donation involves the donation of one of a paired organ (such as kidneys) or a portion of an organ (such as a lobe of the liver or lung).
_
- Deceased organ donation operate under the dead donor rule (DDR), which stipulates that organs may not be removed prior to death nor may organ procurement cause or hasten death. Dead donor rule requires that the intended donor be declared dead before the removal of any life-sustaining organs. Deceased donation is considered only after all life-saving methods to save a patient’s life have been tried. The most common reason for not signing up to be an organ donor is perception that doctors won’t treat them properly if they are in the hospital or emergency room. For decease donation, those responsible for determining death should be completely separate from those assessing feasibility of donation, in order avoid perception that efforts to save lives are reduced in favour of procuring organs. Ordinarily we do not think that persons are dead when we have reasons not to revive them, but only when they cannot physically be revived. Nonetheless, declaring persons dead for purposes of transplantation by DCD criteria is “accepted medical practice” in many parts of the world. So DCD does violate DDR.
_
- There are three methods for determining voluntary consent for deceased organ donation: “opt in” (only those who have given explicit consent are donors); “opt out” (anyone who has not refused consent to donate is a donor); and required request program that encouraged voluntarism by requiring that family members or guardians be given the opportunity to make an organ donation when death has occurred. In terms of an opt-out or presumed consent system, it is assumed that individuals do intend to donate their organs to medical use when they expire. Opt-out legislative systems dramatically increase effective rates of consent for donation as a consequence of the default effect. In a study done to determine if health policy change to a presumed consent or opt-out system would help to increase donors, an increase of 20 to 30 percent was seen among countries who changed their policies from some type of opt-in system to an opt-out system. However, opt-out schemes don’t always translate to increased organ donor rates.
_
- Many feel that they don’t need to donate because thousands of others do. Not all people who die can be organ donors. In the case of people who die of brain death or cardiac death in hospital ICU, they can donate all tissues and many organs (kidneys, liver, lungs etc.). However, most people die due to cardiac arrest outside hospital setup regardless of the condition or situation that causes the heart function to stop. For these cases, they can only donate tissues such as corneas. Remember, only 0.3 to 1 % people die in the way that allows for organ donation. Even if you are a registered organ donor, but if you die of cardiac arrest outside hospital setup, you cannot donate organs. It is only possible to donate organ if you die in hospital or near hospital/transplant center. The fact that organ donation is so often impossible is what makes it so important that as many people as possible register to become donors.
_
- Anyone cannot be organ donor but anyone can register as a prospective donor. Surgeons recover organs from patients with beating hearts (DBD) or just stopped beating before them (DCD). Surgeons don’t recover vital organs from donors who are completely dead and whose hearts have stopped beating as such organs have suffered ischemic damage. Anyone with HIV, severe infection, and actively spreading cancer will be excluded, even when the condition is discovered after death or while a donor is still alive. In the U.S. it legal for HIV-positive individuals to donate organs to HIV-positive recipients.
_
- There is a difference between prospective donor and potential donor. Potential donors are patients who died in hospitals and who are clinically eligible to be organ donors. Prospective donors are living people who are registered for organ donation after their death in opt-in system or those who have not opted out in opt-out system. Prospective donors become potential donors after death (brain death or cardiac death) if they die in right circumstances that allow organ donation. Actual donors (living or non-living) are those with at least 1 organ successfully transplanted into a recipient.
_
- The chances of you needing an organ donation are much higher than the chances of being able to donate once you die. Transplant Priority for Willing Donors is a newer method and the first to incorporate a ‘non-medical’ criterion into the priority system to encourage higher donation rates in the opt-in system. The policy applies nonmedical criteria when allowing the individual who has previously registered as an organ donor, or family has previously donated an organ, priority over another possible recipient.
_
- In nearly all countries with presumed consent laws (opt-out system), donation professionals almost always still seek family consent as if they were in opt-in system. Prospective organ donors must convey their wish to donate organ after their death to their families as almost 90% of families agree to organ donation if they know their relative’s wish but this falls to less than 50% if they haven’t had the conversation. Family can refuse organ donation after death of a prospective organ donor in many countries no matter opt-in or opt-out system.
_
- Living donor can donate one kidney, part of liver/lung/pancreas and donate some tissues like skin, bone and bone marrow. DBD donor can donate heart, lungs, kidneys, liver, pancreas and intestine and tissues. DCD donor can donate kidneys, lungs, liver, pancreas and tissues.
_
- Spain has achieved world’s highest rate of deceased organ donation at 40 donors per million population per year. In contrast, India’s rate of organ donation is a dismal 0.34 donors per million population per year. Simply put, only 1 out of approximately 3 million people in India donates organs after death every year. Netherlands, Turkey, Norway, and the USA now carry out over 20 donations per million population (DPMP) living donor kidney transplants per year; in the UK, the figure is 15.9 DPMP, whereas in Spain and France, the rate is ∼5 DPMP. Spain has the highest deceased donor rate but that does not translate into the highest transplantation rates because of their low rate of living transplantation and their poor rate of utilisation of deceased donor kidneys.
_
- Among transplanting countries, provision of deceased donor transplantation remains significantly associated with gross national income per capita. This reflects the extra resources and organization needed to support deceased donor transplantation, including the requirements for a waiting list and allocation system, an organ procurement programme, an on-call transplantation team and relevant intensive-care resources. There are huge geographical differences on transplant activity ranging from >70 per million population (pmp) per year in developed countries to 0–2.4 pmp in developing countries according to one study.
_
- Living donation makes a significant contribution to kidney (and to a lesser extent liver) transplantation programmes worldwide and carries a number of advantages. Transplantation becomes elective and can be scheduled to the time the patient needs the transplant. Furthermore, the outcomes are better than if a deceased donor organ is used. Live donor kidney lasts about 15-20 years, while the average deceased donor kidney lasts 10-15 years. However, this is at a cost. The mortality rate for living kidney donors is 0.03%, while for living liver donors is 0.2 to 2 %. Living donation also opens the opportunity to commercialization and trafficking. Persons who have donated a kidney for transplantation should avoid high protein diet and limit their protein intake to less than one gram per kilogram body weight per day in order to reduce the long-term risk of chronic kidney disease. Women who have donated a kidney have a higher risk of gestational hypertension and preeclampsia than matched non-donors with similar indicators of baseline health.
_
- Tissue may be recovered from donors who die of either brain or cardio-circulatory death in hospital or cardiac death outside hospital within 24 hours past the cessation of heartbeat provided the body has been refrigerated. Because of three factors—the ability to recover from a non-heart beating donor, the ability to bank tissue, and the number of grafts available from each donor—tissue transplants are ten times more common than organ transplants.
_
- Preservation of cells is dependent on the complexity of their function. The more complex the function the lesser time the organs can be preserved outside the body. In the absence of a circulation, cells rapidly switch from aerobic to anaerobic metabolism, which requires 19 times more glucose substrate to generate adenosine triphosphate (ATP) than aerobic metabolism. The result is rapid consumption of energy substrate, depletion of intracellular energy stores, and accumulation of toxic metabolites and lactic acid. As ionic membrane pumps fail for lack of ATP, the cell membrane depolarizes as sodium enters and potassium leaves the cell. Eventually, cellular integrity is lost. The purpose of organ preservation is to prevent or arrest these changes as quickly as possible. This is achieved primarily by cooling: metabolic rate is halved at temperatures below 10°C, and at 4°C is <10% of that at normal body temperature. As living organ deteriorates rapidly when it loses its blood supply, it needs to be cooled and transported for implantation into the recipient within a limited number of hours. The use of machine perfused organs during storage allows oxygenated fluid to circulate in the tissues, allowing the cells to continue metabolism and help prevent ischemic injury. In a randomized study, cadaveric kidneys stored with machine perfusion had better outcomes than with simple cold storage. Unlike organs, most tissues (with the exception of corneas) can be preserved and stored for up to five years, meaning they can be “banked”.
_
- Warm ischemic time is the time a tissue, organ, or body part remains at body temperature after its blood supply has been reduced or cut off but before it is cooled. Cold ischemic time refers to the time between the chilling of a tissue, organ, or body part after its blood supply has been reduced or cut off and the time it is warmed by having its blood supply restored. The overriding objective with all organ transplantation is avoidance of warm ischemia and reducing cold ischemia. In fact any period of cold or warm ischemia is undesirable. Different organs exhibit different tolerances to warm and cold ischemia, in part related to the nature of the organ and in part because of the demands on the organ after transplantation.
_
- The organs retrieved from DCD donors are exposed to a more prolonged period of warm ischaemia than those retrieved from DBD donors. The extra warm ischaemic damage suffered as a consequence of DCD donation resulting in poor outcome. In the last two decades of organ transplantation, the focus has been on improving immunosuppression to achieve prolonged graft survival. Today, the emphasis has changed and organ preservation is being revisited in an attempt to improve outcomes. This has been spurred on by the rapid increase in DCD donation, and the use of more organs from older donors.
_
- Time is of the essence in organ transplant from deceased donor as kidneys and livers can last up to 24 hours and 10 hours respectively outside the body before being implanted, and for hearts, the transplant must be performed within four hours of the organ being secured. Far more organs are donated than used because even the best preservation technologies can’t stop organs from deteriorating within hours after removal as the whole transplant process takes time. First, tests are run to make sure that organs are immune compatible with potential recipients. Often, the donor’s family must give consent for organ recovery. Then there are the logistical problems and time lost in transport. We need to develop biotechnologies that allow organ banking (cryobanking). In theory, organ banking could be done by freezing and then restoring organs as needed. Immune-matched organs could be supplied in a timely manner to patients at a reasonable cost. The ability to cryopreserve organs would result in numerous lives saved, better medical outcomes, lower costs, faster medical progress, and even better emergency transport systems, including UAV-based ambulances (ambulance drone).
_
- Organ transplantations are incredibly expensive, so transplantation is done for those who can afford them rather than those who need them the most especially in developing countries. Conceptually, donated organs do not belong to the hospital or the city where the donor’s death took place; all altruistic donations belong to society as a whole. Thus the state has a responsibility to ensure that such organs are distributed in a transparent and equitable manner to those who need them the most, and not to those who can afford them. Organs should be allocated to transplant recipients in a fair, equitable process that takes no account of race, religion, gender, social status, disability or age – unless age is relevant to the organ matching criteria.
_
- Transplant rejection occurs when the immune system of the transplant recipient rejects the transplanted tissue; Graft-versus-host disease (GVHD) occurs when the donor T cells reject the recipient tissues. Transplant rejection or allograft rejection is a normal process in which the functional immune system of a transplant recipient attacks the transplanted organ or tissue. Rejection is the major barrier to successful transplantation.
_
- Transplantation antigens include the MHC (major histocompatibility complex) molecules, minor histocompatibility antigens, ABO blood group antigens, and monocytes/endothelial cell antigens. The Rh antigen does not function as a “transplantation antigen,” because it is only present on the surface of red blood cells and not on the parenchymal cells of the graft.
_
- MHC gene system control HLA. The main function of the MHC gene complex is peptide presentation to the immune system to help distinguish self from non-self. These antigens are called HLA (human leukocyte antigens). The principal target of the transplantation immune response is the MHC molecules (HLA antigens) expressed on the surface of donor cells. The degree of similarity between the MHC genes of the donor and recipient is known as histocompatibility; the more genetically compatible the donor and the recipient, the more tolerant the recipient’s immune system should be of the graft. HLA testing in transplant programs include HLA typing of the recipient and the donor, screening of HLA antibodies in the recipient, and detection of antibodies in the recipient that are reactive with lymphocytes of a prospective donor (cross-matching). Tissue typing of recipient and donor determines their human leukocyte antigen (HLA) match. A six-antigen (HLA-A, HLA-B, and HLA-DR from each parent) match confers a graft survival advantage compared with 0 antigen matches for both cadaveric and live donor transplantation.
_
- There is a clear relationship between the degree of HLA matching and kidney graft survival in transplants from living-related donors. Simultaneous analysis of 5,262 one haplotype-matched living-related allografts, and 973 HLA identical allografts showed 10-year projected survival rates of 52% and 73% and graft half-lives of 11.9 and 23.6 years, respectively. The influence of HLA matching on the survival of liver and thoracic organs is yet uncertain. Data from the Collaborative Transplant Study indicate a 1-year graft survival rate of approximately 50–60% following cadaveric ABO-incompatible kidney, liver or heart transplantation, compared with 70–80% for an ABO-compatible organ.
_
- Red blood cells have significantly less MHC molecules per cell. That is why blood transfusions are more successful than organ transplants when both are ABO compatible.
_
- HLA matching has had the greatest clinical impact in kidney, pancreas and bone marrow transplantation, where efforts are made to match at the HLA-A, -B, and -DR loci. In heart and lung transplantation, although studies have shown it would be an advantage to match especially at the DR locus, practical considerations (ischemic times, availability of donors, clinical need of recipients) make this less of a consideration. HLA matching is not required for liver transplants and so not done in centers worldwide. Corneal grafts are not usually influenced by HLA matching, unless being transplanted into a vascularized (or inflamed) bed. With evolving clinical practice, including the provision of safer and more potent immunosuppressive therapy, the significance of HLA matching has diminished. Non-immunologic factors continue to impede more marked improvements in long-term graft survival.
_
- Even when someone is ‘well matched’ with their transplant kidney (in terms of blood group and tissue type), some degree of rejection (approximate risk is 15 out of 100 transplants) is common. Although HLA matching significantly improves the success rate of clinical organ transplantation, it does not by itself prevent rejection reactions. There are two main reasons for this. First, HLA typing is imprecise, owing to the polymorphism and complexity of the human MHC and second, differences between minor histocompatibility antigens. Grafts between HLA-identical siblings are also rejected, albeit more slowly, unless donor and recipient are identical twins. Thus, unless donor and recipient are identical twins, all graft recipients must be given immunosuppressive drugs to prevent rejection. Indeed, the current success of clinical transplantation of solid organs is more the result of advances in immunosuppressive therapy than of improved tissue matching.
_
- ABO compatibility is of much less importance than MHC compatibility in graft survival. However, ABO incompatibility can result in hyperacute rejection of primarily vascularized grafts, such as kidney and heart. ABO incompatible kidney transplantation has become a routine procedure with graft survival rates comparable to the rates in compatible transplantations. Desensitization is usually achieved by plasmapheresis and B cell-depleting therapies that are accompanied by powerful immunosuppression.
_
- Activation of elements of the innate immune system, triggered as a consequence of tissue injury sustained during cell isolation or organ retrieval and ischemia reperfusion, initiate and amplify the adaptive response. Allograft rejection results from the coordinated activation of alloreactive T cells and antigen-presenting cells (APCs). The phenomenon by which the recipient immune system reacts with donor antigens that are considered to be “non-self” is named allorecognition. Allorecognition is initiated by CD4+ and CD8+ T cells recognizing either intact allo-MHC molecules (MHC class II and I, respectively) on donor antigen-presenting cells (APCs) (direct pathway) or allopeptides bound to self-MHC molecules on recipient APCs (indirect pathway) where presentation may occur via MHC class I or MHC class II, although class II is usually involved. Hyperacute rejection occurs due to preformed antibodies against HLA and ABO antigens, acute rejection occurs due to direct allorecognition of non-self HLA antigens and chronic rejection occurs due to indirect allorecognition of non-self HLA antigens. HLA-DR mismatch effect is the most important in the first 6 months after transplantation, the HLA-B effect emerges in the first 2 years, and HLA-A mismatches have a deleterious effect on long-term graft survival. Mismatching of MHC-II provokes more rapid and severe rejection than mismatching of MHC-I antigens.
_
- Pre-existing alloantibodies to blood group antigens and polymorphic MHC antigens can cause rapid rejection of transplanted organs in a complement-dependent reaction that can occur within minutes of transplantation. This type of reaction is known as hyperacute graft rejection .This is an irreversible event, and the only treatment option is immediate graft removal. Today, this type of rejection is avoided in most cases by checking for ABO compatibility and by excluding the presence of donor specific anti-HLA antibodies (DSA) by cross-match techniques between donor lymphocytes and recipient sera. Presence of a positive T-cell CDC (complement-dependent cytotoxicity) crossmatch to the donor is highly predictive of hyperacute rejection.
_
- Acute rejection manifests commonly in the first 6 months after transplantation. The highest incidence of acute rejection is shown after lung, heart, and intestinal transplantation (~35%–40%, 30%–45%, and 55%, respectively). Liver and kidney transplantation generally shows less frequent episodes of acute rejection, with incidences of 13%–30% and 12%–14%, respectively Acute rejection is thought to result from two immunological mechanisms that may act alone or in combination: (1) a T-cell-dependent process that corresponds to acute cellular rejection, and (2) a B-cell-dependent process that generates the acute humoral rejection. IgG antibodies against class I (HLA-A and HLA-B) antigens are highly associated with acute rejection. With current immunosuppressive treatment, acute rejection occurs in less than 15% of the transplants in nonsensitized patients.
_
- Chronic rejection develops months to years after acute rejection episodes have subsided. The use of immunosuppressive drugs and tissue-typing methods has increased the survival of allografts in the first year, but chronic rejection is not prevented in most cases. Chronic rejection appears as fibrosis and scarring in all transplanted organs, but the specific histopathological picture depends on the organ transplanted. For the most part, it is irreversible and eventually results in allograft failure. This process is usually treatment-resistant, although progression may be slowed by immunosuppressive regimens.
_
- Despite the high HLA content of blood transfusions or perhaps because of it, blood transfusions often do not often elicit an antibody response in naive recipients. High sensitization (HLA antibodies) occurs almost always when blood transfusions are given after pregnancies or graft loss. Misconceptions, like erythrocytes do not express HLA antigens, transfusions induce only HLA antibodies against the transfusion donor or leukocyte‐reduced blood is the solution to transfusion‐induced sensitization, make situation worse. Prevention of sensitization will require a more active effort to avoid blood transfusions, whenever possible especially in patients with previous pregnancies or transplants. When such patients need to be transfused, using HLA‐matched blood or immunosuppression, are the options to be considered.
_
- Regulatory T cells (Treg cells) are the counterbalance to aggressive, activated T-cells. Treg cells are critical to the tolerance of an allograft. The more Treg cells present in circulation, the weaker the attack against the transplanted tissue.
_
- Hyperacute rejection is preventable but not treatable, acute rejection is preventable and treatable, chronic rejection is neither preventable nor treatable. Chronic rejection is now the leading cause of graft rejection and most significant medical obstacle to long term morbidity-free allograft survival.
_
- Besides HLA & ABO matching and prior sensitization; survival rate of transplanted organs depend on several factors; including race, size, age, weight, sex/gender, patient’s aftercare, possibility of chronic rejection, how effectively the organ was cooled, how long it took for the organ to reach the recipient, overall health of the donor and recipient, the state of the organ or tissue at the time of recovery and most importantly type of immunosuppressant given to recipient.
_
- Transplantation rejection monitoring aims to increase the survival rate of transferred organs through forecasting and early diagnosing any immunological rejections after an organ transfer, and optimize the use of immunosuppressant to reduce its side-effects. Until now, only invasive method biopsy of transplanted organs was examined which is costly and accompanies by various side effects. Researchers are currently developing non-invasive methods for monitoring rejection of organ transplants. These are transplant biomarkers in the blood or urine that can be used as an initial non-invasive test before resorting to a biopsy. These biomarkers, typically nucleic acids and proteins, could help indicate when a transplanted organ has started to fail, help guide treatments, minimize the number of biopsies needed, and ultimately improve transplant success rates. Biomarkers that indicate how a person’s immune system is functioning could help guide doctors in prescribing the correct dose of immunosuppressants for individual transplant patients to help ward off rejection and minimize side-effects of immunosuppressants.
_
- Cell-free donor DNA in recipient plasma can be used to detect an organ-specific signature that correlates with rejection, and this measurement can be made on any combination of donor and recipient. Because donor DNA can be detected earlier than other rejections signals, physicians might use that information to increase immune suppression to get ahead of a rejection event before it happens, keeping both the transplanted organ and the patient recipient healthier.
_
- Immunosuppressant in organ transplant basically target lymphocytes and are used for:
- Preventing organ rejection and reverse acute rejection in organ transplantation.
- Prevent and treat graft-versus-host disease.
- Minimise destruction of affected tissues in autoimmune and inflammatory diseases.
The use of any immunosuppressive drug requires a balance between the risk of loss of transplanted organ and the toxicity of the agent. At this time immunosuppressive medications appear to be necessary for the life of the transplanted organ. Some patients with severe resistant infections or malignancy related to immunosuppressant require the discontinuation of these medicines. Infection and cancer can occur not only due to immunosuppression in transplant recipient but also due to transmission from donor via donated organ.
_
- Antibodies formed in the recipients against the transplanted organ play a major role in the graft rejection including hyperacute, acute and chronic rejections. The presence of pre-transplant antibodies against antigens encoded by the HLA (human leukocyte antigen) complex, and specifically those antigens that are expressed by the organ donor [donor specific antibodies (DSA)] in recipients, is strongly associated with hyperacute and accelerated acute rejection. Post-transplant antibodies causing acute and chronic antibody-mediated rejections (AMR) are playing an increasingly critical role in kidney allograft loss and are considered among the most important barriers that limit long-term outcomes. The development of post-transplantation antibodies against non-HLA donor antigens is also associated with rejection and decreased long-term graft survival. Thus these antibodies should be removed from the recipient’s circulation as far as possible. Options for antibody depletion in sensitized patients (pre-transplant antibodies) and reversal of antibody-mediated rejection (post-transplant antibodies) include plasmapheresis with or without antibody adsorption columns; extracorporeal photochemotherapy (ECP); intravenous immunoglobulin (IVIG); monoclonal antibodies, e.g. rituximab (a chimeric monoclonal antibody against the protein CD20, which is primarily found on the surface of immune system B cells), and other immunosuppressive drugs. These strategies deplete the level of preformed antibodies to blood groups or to HLA antigens in the recipient and make the crossmatch result negative. These measures also deplete post-transplant antibodies to reverse antibody mediated rejection. Splenectomy is used in desensitization protocols for ABO-incompatible transplants and for antibody-mediated rejection refractory to conventional treatment.
_
- Transplanting donor bone marrow stem cells into the solid organ recipient creates a hybrid immune system or donor immune system if recipient immune system was knocked off. The transplanted organ is no longer recognized as foreign by recipient immune system as it is partly or wholly ‘self’, inducing immune tolerance of transplanted solid organ, thus obviating life time immunosuppression.
_
- Gene therapy has the potential to eliminate problems associated with immunosuppression by allowing the production of immunomodulatory proteins in the donor grafts resulting in local rather than systemic immunosuppression. Alternatively, gene therapy approaches could eliminate the requirement for general immunosuppression by allowing the induction of donor-specific tolerance.
_
- Natural Compounds like curcumin (turmeric), omega-3 fatty acids (fish oil), resveratrol (peanuts, pistachios, grapes, red and white wine), quercetin (apples, onions, grapes and citrus fruits), green and black tea polyphenols and Vitamin D target pro-inflammatory cytokines involved in transplant immunology, thereby reduce rejection and improve graft survival.
_
- The fetus is an allograft that is tolerated repeatedly: because it occupies a site protected by a non-immunogenic tissue barrier, and it promotes a local immunosuppressive response in the mother. There are several sites in the body that also allow prolonged acceptance of foreign tissue grafts. These are called immunologically privileged sites. These include eyes, testes, CNS and articular cartilage. Medically, a cornea transplant takes advantage of this, so also knee meniscal transplantation.
_
- Organs from old donors elicit a more potent immune response that leads to a faster acute graft rejection with increased vasculopathy. Older transplant recipient exhibit reduced frequency of acute allograft rejection but an increased prevalence of infections and malignancies due to immunosenescence.
_
- Optimal contraception is important to initiate before transplantation in women of childbearing age as peritransplantation period is not the optimal time for pregnancy due to highest use of potentially fetotoxic or teratogenic medications. Compared to the general population, a female transplant recipient has about a three times greater chance of having a baby who is premature or low birth weight.
_
- Obese recipients are more likely to have transplant complications including rejection than non-obese recipients.
_
- Studies on renal transplantation observed that male donor to female recipient combination is an independent risk factor for poor graft survival and significantly higher percentage of H-Y antibody production in the male donor-female recipient population could play a role in this phenomenon. In contrast, other studies reported that female donor to male recipient grafts seems to have a worst prognosis in particular for liver and heart transplantation due to reduced female donor “quality” and unfavorable characteristics of male recipients. So impact of sex mismatch on transplant outcome depends on biological and non-biological factors.
_
- Organ transplant confers a 2- to 4-fold increase in solid organ malignancies and up to a 30-fold increase in lymphoproliferative malignancies compared with the general population. This increased risk seems to be directly related to long-term use of immunosuppression, which can lead to disruptions in normal immune surveillance of malignant cells and also leads to increased risk of oncogenic viral infections, such as Epstein-Barr virus (EBV), human papillomavirus (HPV), and human herpes virus 8 (HHV8).
_
- The rate of skin cancer in patients who have undergone organ transplantation is 27% at 10 years, reflecting a 25-fold increase in risk relative to the normal population. The risk of squamous cell carcinoma is about 100 times higher after a transplant compared with the general population’s risk. In light of this substantial risk, it is strongly recommended that all transplant recipients minimize sun exposure.
_
- The pattern of common infections following organ transplantation varies with the net state of immunosuppression and the epidemiology of infectious exposures. Advances in surgical techniques, organ preservation, and improved postoperative care have contributed to more favorable outcome in these patients. Other factors that have positively impacted infection rates in these patients include pretransplant evaluation by infectious disease experts, vaccination, primary antibiotic prophylaxis, improved diagnostics, pre-emptive antibiotic therapy in high risk patients, and effective infection control practices
_
- Three main issues faced by transplant community are organ shortage, lack of research funding and graft rejection including treatment of antibody mediated rejection, ischemia-reperfusion injury and immune monitoring.
_
- Improved survival rates and the expectation that organ replacement will enhance quality of life have encouraged more doctors and their patients with organ failure to opt for transplantation. The success of transplantation creates a problem that is increasingly difficult to manage, the shortage of organs available for transplantation. Organ shortage leads to deaths and poor quality of life for those on the waiting list. Various strategies have been applied to cope with the ever-increasing demand for organs.
-Promoting living donations
-Expanded criteria donors (ECD)
-Donation after cardiac death (DCD)
-Donation from drug overdose deaths
-Legalised monetary compensation for organ donors
-Opt-out system
-Paired donor exchange
-Alternate Listing Transplantation
-Machine perfusion
-Ex-vivo perfusion
-Cryobanking
-Parenchymal cell transplants
-Tissue engineering and regenerative medicine using stem cell transplants
-Organ engineering
-Bioprinting organs
-Artificial organ transplantation
-Xenotransplantation
_
- Transplant rejections are generally more extreme in xenotransplantation than in allotransplantations, ultimately results in rejection of the xenograft, and in some cases result in the immediate death of the recipient. There has not been great success with xenotransplantation for solid organ transplantation, but researchers and scientists did manage to successfully replace parts, such as skin and heart valves from animals to humans. Genetic engineering has allowed human genes to be inserted into pigs so that their cells, tissues and organs are less likely to be rejected when transplanted into humans. As the risk to the recipient would be small, it is likely that corneas will be the first xenotransplants to be carried out as a clinical trial, perhaps followed soon after by neuronal cell or islet cell transplantation.
_
- Research shows that polymer-based nanoparticles containing siRNA can stifle expression of HLAs on surface of endothelial cells lining blood vessels of donor organ, thus prevent rejection.
_
- Research should be done wherein donated organs are infiltrated or perfused by slow release anti-lymphocyte agents so that local immunosuppression is achieved in transplanted organ without side-effects of systemic immunosuppression. The existence of local immune privilege at some specialized tissues, such as the eye, CNS, or pregnant uterus, supports the feasibility of localized immunomodulation. Antirejection drugs delivered locally to the VCA may reduce the need for systemic immunosuppression with its adverse effects. Inhaled immunosuppression with tacrolimus is a novel strategy after lung transplantation. Experiments on rat liver and kidney transplantation with local immunosuppression showed increase graft survival.
_____
Dr. Rajiv Desai. MD.
June 1, 2018
_____
Postscript:
In India, more than 220,000 patients need a new kidney every year, but only 15,000 kidney transplants were carried out in 2017 due to organ shortage. Recently top Indian leaders went through kidney transplant surgeries quickly from unrelated donor kidneys and authorities gave clearances overnight. While people with clout have to wait for just a few days for a kidney, commoners have to wait for years due to complex medical & legal system and high demand. Indians do not have an equal right to live.
______
80 comments on “ORGAN DONATION & TRANSPLANTATION (ODT)”
Leave a Reply

Hey superb blog! Does running a blog like this require a massive amount work? I’ve very little understanding of coding but I had been hoping to start my own blog soon. Anyhow, if you have any recommendations or tips for new blog owners please share. I know this is off topic but I simply wanted to ask. Thanks a lot!|
You’ve made some really good points there. I checked on the internet to find out more about the issue and found most
people will go along with your views on this website.
I always emailed this web site post page to all my friends, because if like to read it afterward my contacts will too.|
Hi there! This is my 1st comment here so I just wanted to
give a quick shout out and say I truly enjoy reading your articles.
Can you recommend any other blogs/websites/forums that cover the same
subjects? Appreciate it!
Howdy would you mind letting me know which web host you’re using?
I’ve loaded your blog in 3 completely different browsers
and I must say this blog loads a lot quicker then most. Can you
recommend a good hosting provider at a fair price? Cheers, I appreciate
it!
Also visit my blog post http://www.Lottoup.com
Pretty! This has been an extremely wonderful article. Thank you for providing
these details.
I really like and appreciate your article.Thanks Again. Cool.
Very good article. Fantastic.
Im obliged for the article. Great.
Hi i am kavin, its my first time to commenting anyplace, when i read this post i thought i could also make comment due to this good post.|
Looking forward to reading more. Great blog post.Really thank you! Much obliged.
Thanks for sharing, this is a fantastic blog.Much thanks again. Really Great.
Really appreciate you sharing this blog.Really thank you! Fantastic.
I want to to thank you for this great read!! I absolutely loved every bit of it. I have got you saved as a favorite to check out new stuff you post…
I cannot thank you enough for the article post.Much thanks again. Fantastic.
Yes, this is a Good one
Terrific article
Terrific article
I get such a giggle reading these posts. For goodness sake…. LEARN ENGLISH. Copy and Paste people. “Please be thanking to be hello on the website. Much like to be seen! Wonder upon you for your writing. How be that you do it? Allah be Praised!!!” (Good for a laugh 🙂
Everyone loves what you guys tend to be up too. This kind of clever work and exposure! Keep up the very good works guys I’ve included you guys to my blogroll.|
Wonderful work! That is the kind of info that are meant to be shared around
the web. Disgrace on Google for no longer positioning this submit
higher! Come on over and discuss with my site .
Thanks =)
Great! Thank you so much. Keep up the good work.
Why people still use to read news papers when in this technological globe everything is existing on web?
I got this website from my buddy who told me on the topic of this
site and now this time I am visiting this site and reading very informative posts at this time.
Wow, this article iss good, my younger sister is analyzing these kinds of
things, therefore I am going to let know her.
Hello, its nice paragraph about media print, we all be familiar with media is a great source of
facts.
Appreciation to my father who informed me about this website,
this website is in fact awesome.
It’s going to be finish of mine day, however before ending I am reading thisgreat article to improve my knowledge.
Hello There. I found your blog using msn. This is a very well written article. I’ll make sure to bookmark it and return to read more of your useful info. Thanks for the post. I’ll certainly comeback.
There’s certainly a lot to find out about this subject.
I love all the points you made.